Abstract
To review and summarize the health complications known to be caused by the coronavirus disease 2019 (COVID-19) and their pathophysiology. A thorough search was conducted for articles on the complications of COVID-19 from December 30th, 2019 through November 20th, 2020. August using the PubMed, Google Scholar, and World Health Organization (WHO) databases. and it was supplemented with inclusion of pertinent articles till May 30th, 2021 Articles that did not have patient data, those which included data of patients < 18 years of age, studies limited to pregnant patients, and studies limited to only specific co-morbidities and organ dysfunctions were excluded to avoid selection bias and heterogeneity in study population. A total of 108 studies were included in the narrative review. These studies reported numerous complications of COVID-19 with the most common being acute respiratory acute respiratory distress syndrome (ARDS) (19.5%–72%), myocardial injury (13.6%–36%), cytokine storm (5%–10%), acute kidney injury (AKI) (4%–54.7%), acute liver injury (14%–62.4%), and venous thromboembolism (VTE) (4%–20%). Our review extensively illustrates the incidence, predictors, and pathophysiology of respiratory, cardiovascular, immunological, hepatobiliary, coagulative, neurological, and renal complications of COVID-19. Enhancing the host immune responses against viral infection and modulating the inflammatory responses, along with appropriate support of respiratory function; as well as the management of complications involving multiple organ systems potential leading to multi-organ failure, are all important aspects to be considered for the recovery of critically ill patients with COVID-19.
Key words: coronavirus disease 2019, respiratory, systemic, complications, review
INTRODUCTION
The coronavirus pandemic, caused by severe acute respiratory syndrome-coronavirus-2 (SARS-CoV-2) has affected more than 180 million lives and more than 3.8 million people have died because of the complications of this highly contagious infection.[1] The virus was first identified in Wuhan, China, in December 2019.[2] The World Health Organization (WHO) declared the outbreak a public health emergency of international concern on January 30th, 2020, and a pandemic on March11th, 2020. The WHO estimates that serious illness may occur in as many as 13.8% of cases and 6.1% are critical.[3]
The illness caused by SARS-CoV-2 ranges from being asymptomatic to fulminant with relation to multiple risk factors which can result in a fatal outcome.[4,5] Though the virus primarily attacks the respirator y system, various case studies and systematic reviews have reported involvement of neurological, cardiovascular, renal, hematological, gastrointestinal, psychiatric and immunological systems.[6,7,8,9,10,11,12,13,14,15] The immune system in particular becomes hyperactive and typically results in a cytokine storm which has been documented as one of the main mechanisms that cause derangements in other body systems and lead to fulminant cases.[16] In addition, more severe cases can develop sepsis, shock and/or multiple organ failure.
Although targeting the virus to improve outcomes is an important ongoing endeavor, major emphasis is currently placed on managing the symptoms that develop as a consequence of this infection.[17] In order to guide decision making for critical care and reduce mortality from COVID-19, comprehensive knowledge of the complications, pathophysiology, and predisposing factors along with the key points in the treatment are of utmost importance.[18,19,20,21,22,23,24,25,26,27] Currently, there are few studies that have covered complications and treatment guidelines regarding COVID-19 and therefore, our review aims to be a comprehensive summary of respiratory and other complications of COVID-19, and the therapeutic approaches.
METHODS
Literature search
A thorough search was conducted for research articles on the complications of COVID-19 and the treatment approach from December 2019 through May 8th, 2020. Three primary databases were used, Pub-Med, Google Scholar, and WHO. The search strategy used the keywords, coronavirus, COVID-19, complication, treatment, therapy and was comprehensive with cross- checking of reference lists from the articles retrieved. Selected articles were independently reviewed by two authors (S.K. and I.G.). All disagreements were resolved with discussion between the two authors, or with input from a third independent reviewer (K.M.). The review protocol was formulated by a senior investigator (R.K.). Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines[28] were used (Figure 1).
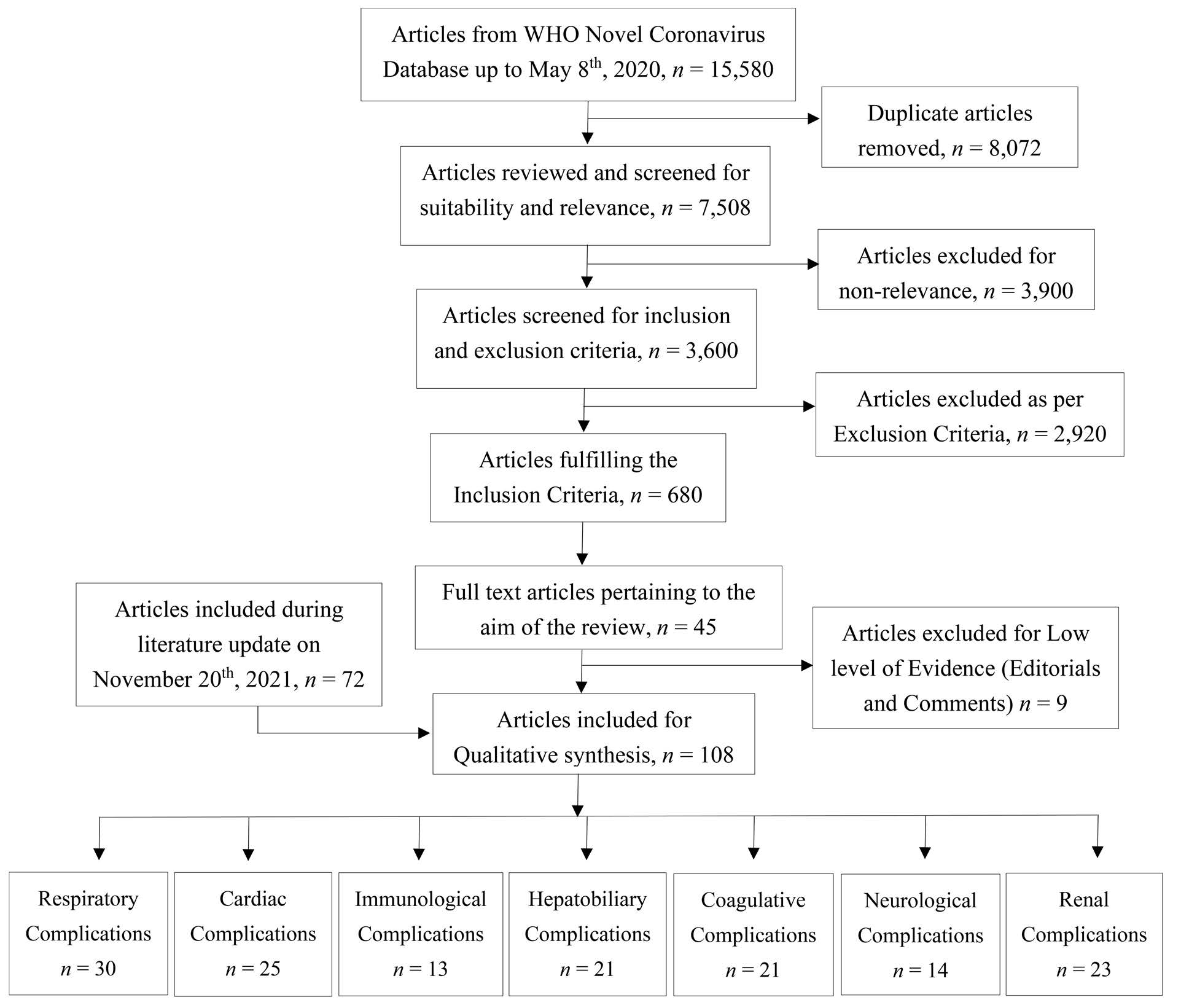
Figure 1: Consort diagram of included studies in review. WHO: World Health Organization.
Inclusion criteria
The final review articles fulfilled the following criteria:
- 1. Reported complications in COVID-19 positive patients and treatment.
- 2. Full text, peer-reviewed articles (Meta-analysis, case-studies and case series, systematic reviews, randomized controlled trials).
Exclusion criteria
Articles which did not have patient data, those which included data of patient <18 years, studies including the pregnant patients, and those limited to specific co- morbidities and organ dysfunctions were excluded to avoid selection bias.
CURRENT KNOWLEDGE OF COMPLICATIONS OF COVID-19
Respiratory complications
Incidence
Acute respiratory distress syndrome (ARDS) is one of the most common complications of COVID-19 infection with more than 3000 reported PubMed indexed articles to its credit. Patients diagnosed with ARDS have a poor prognosis and higher mortality. In a case-series by Wang et al., the time from disease onset to development of dyspnea and development of ARDS was 8 and 10.5 days, respectively.[17]
Two smaller studies reported the incidence of ARDS in COVID-19 as 29%[17] and 41.8%[29] whereas a larger study of 3,062 COVID-19 patients by Zhu et al. reported a 19.5% incidence rate of ARDS in hospitalized patients.[30] The fatality rate in these patients that developed ARDS in the larger study was 5.5%[30] and others reported a high fatality rate in the range of 52.4%-65%[31,32] Among intensive care unit (ICU) patients, 30% of cases had severe lung edema, dyspnea, hypoxemia or ARDS.[32] In a COVID-19 positive population in Wuhan, China, 71% of patients required mechanical ventilation[33] and the estimated mortality is as high as 66% in these patients.[29]
Predisposing factors
Wu et al. found that factors associated with an increased risk of ARDS development in COVID-19 patients were age ≥65 years old), fever ≥39 °C, comorbidities, and lab abnormalities including neutrophilia, lymphocytopenia, elevated organ-specific function tests such as AST and urea, elevated acute phase reactants and elevated coagulation hypercoagulability tests.[29]
Pathophysiology
SARS-CoV-2 belongs to the coronavirus family whose mechanism of infection has been studied for several years. The coronavirus spike protein uses the angiotensin converting enzyme 2 (ACE2) receptor found on the surface of many tissues including the lung, which simultaneously suppresses the ACE2 function and allows entry of the virus into the host, causing lung inflammation.[34,35] Lung inflammation is characterized by leukocyte and neutrophil infiltrates which results in lung endothelial barrier dysfunction characterized by tissue edema, and tissue injury by alveolar wall damage.
Additionally, this inflammation is thought to be a result of the overproduction of inflammatory factors which cause increased vascular permeability and worsening hypoxemia.[32] A clear picture of the pathophysiological changes associated with COVID-19 was demonstrated with the post-mortem lung findings of a 50 years old patient which showed alveolar damage characterized by desquamation of pneumocytes, pulmonary edema, hyaline membranes, and fibromyxoid exudates.[36]
Treatment
Some studies have postulated that the treatment of ARDS with angiotensin Ⅱ will theoretically disr upt angiotensin converting enzyme function, preventing binding of Sars-CoV-2 to receptors.[37] Additionally, stimulation of ACE2 receptors can induce an anti- inflammatory response, cause vasodilation, and reduce oxidative stress in the pulmonary system.[32] Tocilizumab has been shown to be associated with reduction in the biomarkers of COVID-19.[38] Antivirals like Lopinavir/ ritonavir were initially thought to be potentially effective, but their efficacy has not been documented clearly as the supportive evidence is lacking.[39]
More recently, the RECOVERY trial showed a mortality benefit with the use of oral/iv dexamethasone in patients receiving ventilatory support or receiving oxygen without mechanical ventilation; along with a decrease in hospital length of stay- especially in mechanically ventilated patients.[40] smaller observational study reports that a prolonged course of low-dose methylprednisolone initiated early in the clinical course showed a reduction in mortality and ventilatory dependence.[41] A cohort study of 201 COVID-19 patients also found a statistically significant decreased risk of death in those who had developed ARDS and were treated with methylprednisolone as compared to those not treated with methylprednisolone (hazard ratio [HR], 0.38).[29]
Per a recent trial involving 1062 participants, antiviral treatment with remdesivir in patients who were hospitalized and had a lower respiratory tract infection helped in shortening the time to recovery. They also had a lower incidence of new invasive mechanical ventilation requirements with no significant mortality benefits as compared to placebo.[42] In addition to targeting the virus, the hyperactive immune system and inflammatory mechanism should be counteracted. One such strategy includes neutralizing Interferon gamma (IFN-γ) since this inflammatory cytokine is present at high concentrations in the lung of COVID-19 ARDS patients.[37] This can be done with the use of multipotent stem cells with pre- treated IFN-γ to repair damaged lung tissue and vitamin B3 for preventing lung tissue damage as trials have shown this to be beneficial in bleomycin-induced lung injury.[43] Additionally, secondary bacterial pneumonia has been reported in these patients and therefore high-dose vitamin C can be considered in addition to antibiotics.[44]
A study has reported higher levels of tissue factor and plasminogen activator inhibitor-1 in the plasma in patients with ARDS, suggestive of the role of the coagulation system in the pathogenesis of ARDS. Therefore, it is important to address the coagulation system when treating respiratory complications of COVID-19. This is supported by a case series of 3 patients who received alteplase administration and subsequently developed an improvement of Partial pressure of oxygen (PaO2)/Fraction of inspired oxygen (FiO2) ratio ranging from 38%-100% improvement.[45] These findings are similar to the results from a the study by Thachil et al., which showed a reduction of the 7-day and 28-day mortalities by 48% and 37%, respectively in those treated with prophylactic dose of low molecular weight heparin (LMWH) within the initial 7-day onset of ARDS.[46] Also, prone positioning has been recognized as a potential effective treatment for refractory hypoxemia.[47]
Another important aspect in the management of ARDS in patients with COVID-19 infection is airway maintenance and management of hypoxemia. Studies have shown that 50%of all COVID-19 patients required some form of oxygen therapy, including nasal catheter oxygen inhalation, invasive, or non-invasive mechanical ventilation (NIV), or extracorporeal membrane oxygenation (ECMO).[32] When considering oxygen supplementation for patients with hypoxemia, it is important to consider high-flow nasal oxygen which might avoid the need for more invasive ventilation methods as it provides sufficiently high concentrations of humidified oxygen, and facilitates carbon dioxide elimination, also lowers the levels of positive end- expiratory pressure.[44] However, Wang et al. reported a 41% failure rate with high flow nasal cannula use.[48]
Initially, studies did not favor the use of NIV, such as continuous positive airway pressure (CPAP) and bi-level positive airway pressure (BiPAP), in these patients due to increased risk of aerosol generation and lung damage with high tidal volumes and pressures. However, more recent studies support the use of NIV, claiming that 50% of patients who received CPAP did not require invasive ventilation.[49] NIV is reported to have a 29% failure rate.[48] ECMO can be considered in refractory hypoxemic cases using the inclusion and exclusion criteria of the ECMO to Rescue Lung Injury in Severe ARDS (EOLIA) trial,[37] however, its role is not clear and patients must be referred to expert centers that can provide this form of therapy.[50,51]
If the above ventilation therapies do not control hypoxemia, mechanical ventilation can be used, and the National Institute of Health and Care Excellence (NICE) algorithm should be followed. It is recommended that when using mechanical ventilation, adults can receive 6 mL/kg tidal volume with a maximum of 8 mL/kg if the initial volume is not tolerated and children can receive 3-6 mL/kg tidal volume which may be increased to 8 ml/kg if not tolerated. Also, plateau pressure <30 cmH2O in adults and <28 cmH2O in children should be targeted. Generally, positive end-expiratory pressure (PEEP) should be adjusted based on the Fraction of Inspired Oxygen (FiO2) required to achieve the required arterial oxygen saturation (SpO2) and early airway pressure release ventilation should be considered in certain patients. Prone ventilation should last 12-16 hours a day and this should be considered early in patients who lack improvement after optimum ventilator settings of PaO2/FiO2 < 150. Permissive hypercapnia may be considered if hemodynamically satisfactory parameters are maintained as opposed to forms of ventilation which may cause further lung damage.[52,53] Razonable et al. proposed the neuromuscular blockade to decrease metabolic demand as well as to prevent ventilator asynchrony in the patients with moderate or severe ARDS.[6]
Additionally, plasma transfusion should be considered to decrease the need for ventilation and to improve respiratory complications in COVID-19. This is suggested in a case series of critically ill patients by Shen et al. who noted that within 4 days of Plasma transfusion, ARDS was resolved and 3 patients were weaned off ventilation within 14 days of treatment.[54] However, some studies have denied the beneficial effect of convalescent and further studies are needed to prove its efficacy.[55]
The last resort for the management of respirator y complications in COVID-19 patients is with surgical measures. Lang et al. and Chen et al. resorted to managing bilateral lung damage secondary to COVID-19 via a successful double lung transplant and therefore this can be considered in severe cases and with an experienced team.[56,57] (Table 1)
| Systemic Complication | No. of related articles | Incidence (Range) | Mortality (Range) | Predisposing Factors | Pathophysiology (Points) | Treatment (Points) |
| Respiratory complications-Acute Respiratory Distress Syndrome (ARDS), Respiratory Failure, Acute Lung Injury | 21 (6, 17, 29-32, 34, 36, 37, 42-46, 48-50, 52,54, 64, 103) | 19.5%-29% ARDS[17,29,30] | 5.5%-65% ARDS[29,31,32] | Age ≥65 years old, Male, fever ≥39 °C, Smoking comorbidities, neutrophilia, lymphocytopenia, elevated AST and urea, elevated acute phase reactants and elevated coagulation hypercoagulability tests[29,33,64] | Angiotensin converting enzyme 2 (ACE2) receptor allows entry of the virus into the host, causing lung inflammation resulting in overproduction of inflammatory factors which cause increased vascular permeability and worsening hypoxemia[32,34,36] | Angiotensin II, glucocorticoids, antiviral, anti-inflammatory agents, multipotent stem cells, antibacterial for secondary infection, low molecular weight heparin (LMWH), ventilator mechanisms and lung transpla nt[6,29,34,37,42-46,48-50,52,54] |
| Cardiac Complications-Myocarditis, cardiac tamponade, myocardial infarction and microangiopathy, Cardiac Failure | 10 (6, 21, 31, 60, 62, 64, 65, 67, 69, 70) | 1%-15% of survivors, 28%-46% of non-survivors[31] | Not reported | Underlying cardiovascular disease such as hypertension, coronary heart disease and cardiomyopathy[60,62,64] | Systemic inflammatory response can lead to vascular inflammation and atherosclerotic plaque dislodgement or rupture - respiratory complications of coronavirus disease 2019 (COVID-19) can induce hypoxia and cause cardiac injury[60,64,65] | - Agents considered include antiplatelet agents, β-blockers, ACE inhibitors, and statins - Cardiac complications require rapid diagnosis and management. Diagnostic modalities should limit use among other patients to prevent widespread nosocomial infections. The advantage of mechanical circulatory support should be weighed against coagulopathy risks[6,64,67,69,70] |
| Immunological complications - Cytokine Storm | 6 (6, 16, 73, 77, 80, 81) | 5%-10%[6] | 27%[73] | Not reported | Cytokine storm is characterized by an excessive and aberrant immune response associated with severe multi-organ pathology. Elevated levels of chemicals associated with inflammation, lymphocytopenia, reduced T cells and natural killer cells are noted[16,76,103] | Recommended treatment includes anti-inflammatory medication, tocilizumab (monoclonal antibody against IL-6R) and artificial-liver blood-purification systems in severe cases[16,77,81] |
| Hepatobiliary Complications - Hepatic Failure, Acute hepatitis, Acute Liver Injury | 7 (17, 67, 82, 83, 85, 87, 88) | 14.8%-52%[17,83,85] | Not Reported | Males, Elevated white blood cells, neutrophils, C reactive protein (CRP) and Lung lesions on computed tomography[17,82,83] | The ACE2 receptor expressed on hepatocytes and cholangiocytes are involved with liver damage seen in COVID-19 patients. Binding of the virus to this receptor prevents liver regeneration and immune response[36,87] | - Early admission considered if patients have additional risk factors. - Cirrhosis-associated complications should be managed appropriately. - Drugs known to be toxic to liver should be avoided in these patients or doses should be adjusted accordingly[67,88] |
| Coagulative Complications-Disseminated Intravascular coagulopathy (DIC), Coagulopathy, Thromboembolism, Stroke, Ischemic Limb | 5 (6, 44, 76, 90, 92) | 5%-12% thrombocytopenia, 5% PT prolongation, 36%-59.6% D-Dimer increase, 71.4%-DIC[44,90] | Not reported | Not reported | - Damage to the microvascular system leads to the activation of the coagulation system, systemic microvascular thrombosis, massive consumption of coagulation factors and secondary hyperfibrinolysis - Prolonged immobilization during illness, dehydration, an acute inflammatory state and presence of other cardiovascular risk factors increases risk of coagulation complications - Invasive procedures such as mechanical ventilation, central venous catheterization, and surgery may induce vascular endothelial damage and cause coagulation complications[76,90] |
- Early diagnosis and follow-up using ISTH score - Identify high-risk patients. - LMWH and Unfractionated Heparin preferred over direct oral anti-coagulants (DOAC) [6,90,92] |
| Neurological Complications-Central Nervous System (CNS), Peripheral Nervous System (PNS) and skeletal muscle injury | 5 (64, 97-100) | 36.4%, 20%-Hypoxic encephalopathy[64,97,98] | Not reported | Not reported | - ACE2 receptor is expressed in nervous system and skeletal muscle. - Hyper-activation of various inflammatory cytokines may target neurological tissues and cause damage - SARS-COV-2 may also enter the CNS through the hematogenous or retrograde neuronal route[97-99] |
- Prompt diagnosis of neurological cases due to rapid deterioration - Treatment with either immuno-modulatory therapies, such as methylprednisolone or gamma globulin, hemodialysis or preventive anticoagulation might be beneficial because an increased inflammatory response and coagulation abnormalities may progress to neurological complications[100] |
| Renal Complications-Acute Kidney Injury, Renal Failure | 3 (6, 101, 103) | 0.1%-29%[101] | Not reported | Older age, comorbidities (hypertension, coronary heart disease, chronic kidney disease), hypovolemia, shock manifestations, and the use of nephrotoxic drugs[101] | Coronavirus causes tubular damage in the kidney, leading to abnormalities in urinalysis and impairment of glomerular filtration function This could be the result of direct attack by the virus, immune-mediated injury or excessive apoptosis and mitochondrial stress that leads to sepsis-related Acute kidney injury (AKI)[6,101] | Risk screening, early recognition, timely treatment and renal replacement therapy are the standardized principles for treatment of AKI[103] |
Cardiac complications
Incidence
One study defines cardiac injury as an elevated serum level of high-sensitivity cardiac troponin I greater than 28 ng/mL and results of their research found cardiac injury in 28% of non-survivors and 15% of survivors with COVID-19. Similarly, another study reported cardiac injury in 46% of non-survivors compared to 1% of survivors.[31] These studies suggest that the presence of cardiac injury is associated with increased mortality.[58] Other cardiac complications reported in COVID-19 were heart failure, myocarditis which was reported in a few case studies, cardiac tamponade, myocardial infarction, arrythmias[59] and microangiopathy.[60] The most common arrhythmogenic mechanism is the QT prolongation leading to polymorphic ventricular tachycardia. 61 Heart failure was found in 23% of patients and also had a higher rate in non-survivors as compared to survivors (52% vs. 12%).[31]
Researchers have established that patients with known cardiovascular comorbidities were more likely to develop cardiac complications with COVID-19.[62,63] Also it has been reported that 35% of COVID-19 patients had an underlying cardiovascular disease such as hypertension, coronary heart disease and cardiomyopathy.[64]
Pathophysiology
Viral infections are known to trig ger many cardiac complications such as acute coronary syndromes, arrhythmias and heart failure as a result of a systemic inflammatory response which can lead to vascular inflammation and atherosclerotic plaque dislodgement or rupture.[60,64] This systemic inflammatory response is supported by patients having higher levels of troponin, myoglobin, C-reactive protein, ser um ferritin, and interleukin-6.[58,64] Another mechanism of cardiac damage is by direct invasion of cardiomyocytes by SARS-CoV-2 via the ACE2 receptor.[65] Additionally, considering that respiratory complications of COVID-19 can induce hypoxia, a decreased supply of oxygen to the cardiovascular system may result in its injury.[65]
Treatment
Treatment of cardiovascular complications of COVID-19 should be based on the existing guidelines. As recommended by practice guidelines antiplatelet agents, β-blockers, ACE inhibitors, and statins should be used.[64,66] Additionally, antioxidants have been proposed for the management of cardiac injuries in critically ill COVID-19-infected patients, however the clinical data is unavailable for the same.[67] the efficacy of glucocorticoids and IL-6 inhibitors is debatable.[68]
Guidelines from the European Society of Cardiology[69] state that these steps should be taken in COVID-19 patients with cardiovascular complications:
- 1. Cardiovascular complications should not be overlooked due to a COVID-19 diagnosis and therefore requires rapid diagnosis and management.
- 2. Diagnostic testing modalities appropriate for monitoring cardiovascular complications such as electrocardiogram (ECG), echocardiography (ECHO) and coronary angiography may var y depending on local resources and providers should keep into account ways on how to minimize widespread nosocomial infections. A multidisciplinary evaluation should be done before taking the decision for procedures like coronary angiography based on the severity of illness considering the risk and the benefit from coronary revascularization in patients with ST-segment elevation.[6]
- 3. The advantage of mechanical circulatory support should be carefully weighed against the risk of coagulopathy associated with COVID-19 infection.
- 4. The risk-benefit ratio should also be considered because complications like drug-induced ventricular arrhythmias and sudden cardiac deaths associated with the administration of hydroxychloroquine.[70,71] (Table 1)
Immunological complications
Incidence
The hallmark of the pathophysiology of immunological response to COVID-19 is the cytokine storm syndrome. 5-10 % of the COVID-19 patients develop the critical hyper inflammatory stage associated with end-organ damage, thus resulting as complication.[6,72] Cytokine storm is a crucial cause of death in COVID-19 patients and the mortality resulting from cytokine storm precipitated by the viral infection (SARS-CoV 2) is nearly 27%.[73,74]
Pathophysiology
The coronavirus induced “cytokine storm” causing multi- organ failure is a well-known phenomenon contributing to the high morbidity and mortality associated with the disease. This hyper-cytonemia is a result of increased levels of cytokines/chemokines like interleukins (IL)-1, IL-6, IL-8, IL-12, interferon (IFN)-γ, IFN-γ-induced protein 10 (IP-10), and monocyte chemo-attractant protein-1 (MCP-1) which are associated with inflammation and extensive damage in lungs and other organs. Elevated levels of these inflammatory markers (e.g.: interleukins 2,7, and 10, granulocyte colony stimulating factor [GCSF], MCP-1, macrophage inflammatory protein 1α [MIP1A], and tumor necrosis factor [TNF]-α) are associated with severe COVID-19 infection causing critical illness in patients.[16,75]
In addition to the cytokine storm, lymphocytopenia is another prominent finding in COVID-19 patients. Both T cells and Natural Killer (NK) cells in patients with COVID-19 were found to be reduced. In some critically ill patients, NK cells were extremely low, or even undetectable and T-cells including memory helper T cells and regulatory T cells were decreased in severe cases. Secondary lymphoid tissue destruction has also been noted in COVID patients.[33,76] T he COVID-19 induced cytokine storm causes rapid clinical deterioration and can often be fatal, therefore, timely identification and appropriate management are key in attaining a favorable outcome.
Treatment
Commonly available anti-inflammatory agents, such as corticosteroids, inflammatory cytokine antagonists (such as interleukins-6 receptor [IL-6R] monoclonal antibodies, TNF inhibitors, IL-1 antagonists, Janus kinase inhibitor inhibitors) and intravenous immunoglobulin (IVIG) can be employed to modulate the systemic inflammatory state and prevent multi-organ dysfunction.[77,78]
IL-6 was found to be one of the most important cytokines involved in COVID-19-induced cytokine storms. A monoclonal antibody against the IL-6R, Tocilizumab was recently found to reduce the likelihood of patients not requiring mechanical ventilation to further deteriorate and be placed on mechanical ventilation, however, it showed no mortality benefits when compared to placebo.[79,80]
Some studies reported that the cytokine/chemokine clearance achieved by Artificial-liver blood-purification systems may be effective for treating severely ill patients. These artificial-liver blood-purification systems consist of plasma exchange, plasma absorption, and hemo/plasma filtration. A study done at the First hospital of Zhejiang University found that patients receiving Li’s artificial liver treatment showed shorter ICU stays in the case-series of 3 patients.[16,81] (Table 1)
Hepatobiliary complications
Incidence
It has been observed that patients infected with SARS-CoV-2 may develop different degrees of liver injury, mainly indicated by abnormalities in Alanine Transaminase (ALT), Aspartate Transaminase (AST) and bilirubin. In one particular retrospective study by Xie et al., they found that 31.6%, 35.4% and 5.1% had elevated ALT, AST and bilirubin, respectively. They also concluded that males and those with elevated white blood cells, neutrophils, C-reactive protein (CRP) and having lesions on computed tomography (CT) were more likely to have liver injury and a longer admission period.82 This suggests that liver injury was more common in severe COVID-19 cases, which is consistent with an epidemiological study that reported 62% of ICU patients developing liver injury as compared to 25% of non-ICU patients in the study.[17] In addition, another study found 78% of patients who died of COVID-19 had developed liver injury.[83]
The degree of liver injury may mirror the severity of COVID-19. A review article that aimed to understand livery injury in COVID-19 patients found that the incidence ranged from 14.8% to 53% in the COVID-19 patients studied.[84] They also found decreased albumin in severe cases around 26.3-30.9 g/L.[85] Wang et al. in their case series of 52 patients observed pancreatic injury defined as defined by amylase or lipase abnormality in 17 % of patients.[86]
Pathophysiology
SARS-CoV-2 uses the ACE2 as its entry receptor, which is expressed in hepatocytes and cholangiocytes, with cholangiocytes having a higher concentration of these receptors. One study that identified the expression of ACE2 in liver tissue noted that there was specific expression in cholangiocytes, suggesting direct binding of SARS-CoV2 to cholangiocytes and not hepatocytes could be the culprit of liver damage.[87]
Considering that bile duct epithelial cells play an important role in liver regeneration and immune response, damage to these cells can lead to drastic effects on the liver because it would theoretically not be able to regenerate new cells and compensate for damage caused by the virus.
Pathological changes in the liver were demonstrated in a liver biopsy of a 50-year-old male COVID-19 patient which showed moderate microvesicular steatosis and mild lobular and portal activity. This was believed to be a result of either direct viral infection or drug-induced liver injury.[36]
Treatment
Excessive reactive oxygen species (ROS) will oxidize cellular proteins and membrane lipids leading to hepatocyte damage. Thus, a proper dose of antioxidants may ameliorate hepatic injuries in critically ill COVID-19 patients. However, the definitive evidence is lacking.[67]
Guidelines established by the European Association for the Study of the Liver (EASL) and the European Society of Clinical Microbiology and Infectious Diseases (EASL/ ESCMID)[88] are as follow:
- 1. Early admission should be considered if there are additional risk factors present.
- 2. Hepatic Cirrhosis-related complications like hepatic encephalopathy, portal hypertension, ascites, bacterial peritonitis, and others should be addressed and managed appropriately.
- 3. In patients with Hepatocellular Carcinoma (HCC), loco-regional and immune-checkpoint inhibitor therapies should be postponed when possible and decisions on discontinuing kinase inhibitors in non- severe COVID-19 patients should be addressed individually.
- 4. Hydroxychloroquine, tocilizumab and sofosbuvir use should be preferred over remdesivir and lopinavir/ ritonavir use as they have fewer hepatic interactions. Additionally, baricitinib and anakinra are relatively safer.
- 5. Dose adjustment of calcineurin- and/or mammalian target of rapamycin (mTOR) inhibitors post-liver transplant might be required depending on the antiviral therapy initiated. (Table 1)
Coagulation complications
Incidence
Another hallmark of severe COVID-19 is coagulopathy. 71.4% of patients who die of COVID-19 meet International Society on Thrombosis and Hemostasis (ISTH) criteria for disseminated intravascular coagulation (DIC). COVID predisposes patients to a hypercoagulable and pro- thrombotic state leading to the increased incidence of venous thrombo-embolism (VTE) and DIC in this select population. This can be monitored by elevated D-dimer levels, fibrin degradation products high fibrinogen levels and low anti thrombin levels, and can manifest clinically as pulmonary congestion with microvascular thrombosis and occlusion along with other vaso-occlusive events (e.g. ischemic limbs, strokes, etc.) in critically ill COVID-19 patients.[44,89]
In a review by Wang et al., the incidence of thrombocytopenia was 5%-12%, the proportion of prothrombin time (PT) prolongation is 5%, and the proportion of D-dimer increase is 36%-60%. There has also been a statistically significant difference found between PT prolongation and D-dimer elevation in ICU patients as compared to non-ICU patients.[90]
Pathophysiology
DIC is based on many pathogenic factors including damage to the microvascular system resulting into the hyperactivation of the coagulation cascade, systemic microvascular thrombosis, massive consumption of coagulation factors and secondary hyper-fibrinolysis.[91] This causes clinical syndromes characterized by hemorrhage and microcirculation failure. Patients with COVID pneumonia are immunocompromised and can quickly develop cytokine storms and secondary bacterial and fungal infections. These patients along with those who developed inflammatory factor storms are at higher risk for DIC.[90]
Many critically ill patients have vasculitis-like manifestations including small vessel hyperplasia, vessel wall thickening, lumen stenosis, occlusion and focal hemorrhage. In some cases, gangrene of the extremities has also been noted.[76] The acute inflammatory state induced by this viral illness, along with the prolonged immobilization during hospitalization are both risk factors for this complication. Other factors include dehydration and the presence of other cardiovascular comorbidities. Moreover, Surgery, mechanical ventilation and central venous catheterization may further induce vascular endothelial damage, therefore increasing the risk for deep vein thrombosis (DVT) and eventually leading to pulmonary embolism.[76]
Treatment
ISTH guidance on disseminated intravascular coagulation:[92,93]
- 1. In addition to platelet count, PT and D-dimers, it may be useful to measure fibrinogen in this scenario. It was proposed that using anticoagulation to inhibit thrombin generation in sepsis-associated coagulopathy may prove to be beneficial.[6]
- 2. Keeping a low threshold of suspicion for DIC (which can be diagnosed early by applying the ISTH score: platelet count, PT, fibrinogen, D-dimer, antithrombin and protein C activity monitoring) can help in curating an appropriate treatment plan for critically ill patients and could possibly also have prognostic value.
- 3. Early identification of the at-risk patient population.
Low molecular weight heparins (LMWH) like Enoxaparin, heparin and direct oral anticoagulants (DOACs) are now extensively used in clinical practice to reduce the risk of in hospital VTE. A recent cohort study in December talks about similar mortality benefits of apixaban and enoxaparin in moderate to severely ill COVID-19 patients.[94] Due to possible drug-drug interactions. In COVID 19 patients, the anti-inflammatory characteristics of LMWH could be an added advantage and the potential need to integrate other anti-thrombotic therapies such as anti-thrombin as well as recombinant thrombomodulin could also be valuable in this dynamic phase of ‘immunothrombosis’.[90,95] (Table 1)
Neurological complications
Incidence
Mao et al. evaluated patients infected with COVID-19 and found that 36.4% had nervous system manifestations and they were more common in patients with severe infections. Similarly, Pooya et al. found the incidence of neurological manifestations in 25% of the patients with COVID-19.[96] The most common symptoms reported were, signs of dizziness, headache, diminished consciousness, acute cerebrovascular disorder (either ischemic stroke or cerebral hemorrhage), ataxia and seizures in the central nervous system. Other manifestations were skeletal muscle injury and peripheral nervous system symptoms such as nerve pain, taste impairment, smell impairment and vision impairment. They found that on average, these manifestations occurred in the first two days of the illness and, these neurological symptoms were the presenting complaints in some cases instead of typical COVID-19 symptoms such as fever, cough and diarrhea.[97]
In addition to these, other studies also re por ted COVID-19 neurological complications. A retrospective study done by Tao Chen et al. found that 20% of patients who died of coronavirus had developed hypoxic encephalopathy.[62] Sedaghat et al.. reported Guillain- Barre Syndrome symptoms in one infected patient with COVID-19, which began approximately two weeks after the onset of respiratory symptoms.[98]
Pathophysiology
Although the mechanism of neurological damage in COVID-19 is unclear and requires further research, several logical mechanisms have been devised. Both SARS and COVID-19 attach to the ACE2 receptor which is expressed on the cell membrane of numerous human organs, including lung, kidney, liver, nervous system and skeletal muscle. After attachment to the receptor, the virus stimulates an inflammatory process in the body which causes the production and hyper-activation of various inflammatory cytokines, some that may target neurological tissues and cause damage.[98] During this inflammatory process, the coagulation system can also be damaged and lead to increased risk for cerebrovascular disease. Alternative route of entry for SARS-COV-2 in the central nervous system is either hematogenous or retrograde neuronal route. Other researchers have postulated that although direct damage to neurological tissues is plausible, they believe that indirect damage secondary to underlying comorbidities in patients could also cause various neurological presentations of COVID-19.[99]
As referenced previously, nervous system manifestations were significantly more common in patients with severe infection.[97] With this severe infection, it has been found that these patients can rapidly deteriorate and develop worsening symptoms which can lead to a stroke and contribute to a high mortality rate in these patients.
Treatment
Guidelines for neurological complications are as follow: During early symptomatolog y, prompt diagnosis of neurological cases of COVID-19 and proper monitoring of pre-existing neurological disease is crucial. Also, during this time, it is important to beware of immunological exacerbation and secondary infections which must be addressed promptly to prevent further progression.
Deterioration of severely ill patients, associated with increased inflammatory response and blood coagulation abnormalities, can rapidly develop into neurological complications such as cerebrovascular disease. At this stage, treatment with methylprednisolone, gamma globulin, hemodialysis or preventive anticoagulation for stroke might be beneficial.[100] (Table 1)
Renal complications
Incidence
The kidney is another highly affected organ in severe COVID-19 patients. Acute kidney injury (AKI) in a COVID-19 patient is a risk factor for poor prognosis and it is more likely to occur in severely ill patients. The reported incidence by Cheng et al. of AKI varied from 0.1%-29% in hospitalized patients, where among patients in ICU was found to be 8.3%, while the incidence of AKI among non-ICU patients was 2%.[101] Adapa et al. reported the incidence of acute kidney injury about 3-15% in patients with COVID-19 which significantly increased in patients in the intensive care unit to 15% to 50%.[102]
Pathophysiology
Studies have shown that coronavirus causes tubular damage in the kidney, leading to abnormalities in urinalysis. There is also impairment in glomerular filtration function, which is manifested by increased blood creatinine and urea nitrogen levels. At present, it is speculated that the mechanisms responsible are the direct attack by virus, immune mediated injury causing excessive inflammation and apoptosis, Angiotensin Ⅱ pathway activation and coagulopathy resulting in microvascular thrombosis leads to AKI.[6,101]
Treatment
Yang et al. suggests that there should be a standardized approach to the prevention and treatment of AKI. They have devised a “5R principle” which could be used to improve the prognosis of these patients and it includes risk screening (Risk), early recognition (Recognition), timely treatment (Response), renal replacement therapy (Renal replacement therapy) and renal recovery (Recovery).
- 1. Risk screening: The incidence of AKI in a study of 710 COVID-19 patients was reported as 3.2. Out of these, 50% were diagnosed with AKI grade 2 and 40% were diagnosed with AKI grade 3. Therefore, risk screening can help early intervention and reduce the occurrence or progress of AKI. The high-risk factors for AKI in COVID-19 include older age, history of hypertension, coronary heart disease, chronic kidney disease, hypovolemia, shock manifestations, and the use of nephrotoxic drugs.
- 2. Early recognition and action: the volume and hemodynamics should be optimized to ensure sufficient effective perfusion pressure of the kidneys and avoid the use of nephrotoxic drugs as much as possible.
- 3. Renal replacement therapy: the proportion of continuous renal replacement therapy (CRRT) in patients with COVID-19 ranges from 1.5% to 9%. Among them, CRRT is required for severe and critically ill patients admitted to the ICU. The ratio is 5.6% -23%. The mode is continuous veno-venous hemofiltration (CVVH) or continuous veno-venous hemodiafiltration (CVVHDF). Mainly, but since the fact that cytokine storm is the main cause of organ damage in COVID-19, emphasizing the status of comprehensive blood purification treatment for severe COVID-19: CRRT is not just a kidney replacement during AKI. For severe COVID-19 patients without AKI, when severe cytokine storms and multiple organ dysfunction syndromes (MODS) occur, CRRT may be started at the earliest.[103](Table 1)
STRENGTH AND LIMITATION
Our work serves as a comprehensive and intense summary of complications of the disease which has laid foundation to multiple narrowed research questions and studies on the management of the particular systemic complications which are being submitted to various journals. The data of our study is a grain of salt in the frenzy of new discoveries and clinical trials in order to find the best treatment option for COVID-19.
The limitations of our study are it predominantly describes the clinical data and incidence rates of complications in hospitalized patients. Another limitation was we could not register the review. We tried to prospectively register our review but decided to go against it as it was taking unreasonably longer time than expected due to the increased pool of COVID-19 related articles. Also, our study also relied on data from case-series and clinical trials in early phase, with low level of evidence. Larger scale studies estimating the various systemic involvements are needed to confirm the findings.
CONCLUSION
The treatment protocols for the various systemic complications of COVID-19 are indistinct and need further evaluation. Further clinical research is needed on the efficacy and use of the existing drugs for the treatment of COVID-19 systemic complications. Global observational studies with a large sample size may shed some light on probable causal relationships and possible improved outcomes.[4,104,105] Along with enhancing the host immune responses against viral infection, Monitoring and support of respiratory along with multi-organ function, modulating the inflammatory response individually, as well as the prophylaxis and treatment of complications are be crucial for the recovery of critically ill adult patients with COVID-19.
DECLARATIONS
Funding
None declared.
Conflict of interest
The authors declare no conflict of interest.
REFERENCES
- Organization WH. WHO Coronavirus Disease (COVID-19) Dashboard. 2022. Available at: https://covid19.who.int/?gclid=CjwKCAiAl-4WABhAJEiwATUnEF3GOGkkx7rB8C7kJnB9vVZ_7yx%E2%80%93_a%E2%80%93usfJD-cRCSV5suYX0u%E2%80%931W7zyhoCWSwQAvD_BwE Accessed January 15, 2021.
- Shah A, Kashyap R, Tosh P, Sampathkumar P, O’Horo JC. Guide to Understanding the 2019 Novel Coronavirus.
Mayo Clinic Proceedings 2020;95:646-652. DOI: 10.1016/j.mayocp.2020.02.003 PMID: 32122636 - Keith P, Day M, Perkins L, Moyer L, Hewitt K, Wells A. A novel treatment approach to the novel coronavirus: an argument for the use of therapeutic plasma exchange for fulminant COVID-19.
Crit Care 2020;24:128. DOI: 10.1186/s13054-020-2836-4 PMID: 32241301 - Domecq JP, Lal A, Sheldrick CR, Kumar VK, Boman K, Bolesta S, et al. Outcomes of Patients with Coronavirus Disease 2019 Receiving Organ Support Therapies: The International Viral Infection and Respiratory Illness Universal Study Registry.
Crit Care Med 2021;49:437-448. DOI: 10.1097/CCM.0000000000004879 PMID: 33555777 - Singh R, Rathore SS, Khan H, Karale S, Chawla Y, Iqbal K, et al. Association of Obesity With COVID-19 Severity and Mortality: An Updated Systemic Review, Meta-Analysis, and Meta-Regression.
Front Endocrinol (Lausanne) 2022;13:780872. DOI: 10.3389/fendo.2022.780872 PMID: 35721716 - Razonable RR, Pennington KM, Meehan AM, Wilson JW, Froemming AT, Bennett CE, et al. A Collaborative Multidisciplinary Approach to the Management of Coronavirus Disease 2019 in the Hospital Setting.
Mayo Clinic proceedings 2020;95:1467-1481. DOI: 10.1016/j.mayocp.2020.05.010 PMID: 32622450 - Rathore SS, Rojas GA, Sondhi M, Pothuru S, Pydi R, Kancherla N, et al. Myocarditis associated with Covid-19 disease: A systematic review of published case reports and case series.
Int J Clin Pract 2021;75:e14470. DOI: 10.1111/ijcp.14470 PMID: 34235815 - Sheraton M, Deo N, Kashyap R, Surani S. A Review of Neurological Complications of COVID-19.
Cureus 2020;12:e8192. DOI: 10.7759/cureus.8192 PMID: 32455089 PMCID: PMC7243063 - Khan H, Sabzposh H, Deshpande S, Kashyap R. Pregnancy during COVID-19 pandemic-Maternal and neonatal outcomes: A concise review.
Int J Acad Med 2020;6:287-293. DOI: 10.4103/IJAM.IJAM_94_20 - Shah K, Mann S, Singh R, Bangar R, Kulkarni R. Impact of COVID-19 on the Mental Health of Children and Adolescents.
Cureus 2020;12:e10051. DOI: 10.7759/cureus.10051 PMID: 32999774 - Sheraton M, Deo N, Dutt T, Surani S, Hall-Flavin D, Kashyap R. Psychological effects of the COVID 19 pandemic on healthcare workers globally: A systematic review.
Psychiatry Res 2020;292:113360. DOI: 10.1016/j.psychres.2020.113360 PMID: 32771837 - Singh R, Kashyap R, Hutton A, Sharma M, Surani S. A Review of Cardiac Complications in Coronavirus Disease 2019.
Cureus 2020;12:e8034. DOI: 10.7759/cureus.8034 PMID: 32528770 - Bhalala U, Gist K, Tripathi S, Chiotos K, Dapul H, Gharpure, Varsha3; et al. 145: Pediatric COVID-19: A Report From Viral Infection and Respiratory Illness Universal Study (VIRUS).
Crit Care Med 2021;49:58. - Sandeep T, Katja G, Kathleen C, Heda D, Varsha G, Vikas B, et al. 61: Risk Factors for Severe COVID-19 Illness in Children: Analysis of the VIRUS: COVID-19 Registry.
Crit Care Med 2021;49:32. - Kwenandar F, Japar KV, Damay V, Hariyanto TI, Tanaka M, Lugito NPH, et al. Coronavirus disease 2019 and cardiovascular system: A narrative review.
Int J Cardiol Heart Vasc 2020;29:100557. DOI: 10.1016/j.ijcha.2020.100557 PMID: 32550259 - Zhang Y, Yu L, Tang L, Zhu M, Jin Y, Wang Z, et al. A Promising Anti- Cytokine-Storm Targeted Therapy for COVID-19: The Artificial-Liver Blood-Purification System.
Engineering (Beijing) 2021;7:11-13. DOI: 10.1016/j.eng.2020.03.006 PMID: 32292628 - Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China.
Lancet 2020;395:497-506. DOI: 10.1016/S0140-6736(20)30183-5 PMID: 31986264 - Mehra I, Mahapure K, Armaly P, Mehra I, Mahapure KS, Armaly P, et al. Controversial Role of Corticosteroids on Mortality in COVID-19: Systematic Review and Meta-Analysis.
Crit Care Med ;49:58. - Singh R, Shaik L, Mehra I, Kashyap R, Surani S. Novel and Controversial Therapies in COVID-19.
Open Respir Med J 2020;14:79-86. DOI: 10.2174/1874306402014010079 PMID: 33717367 - Bansal V, Mahapure KS, Bhurwal A, Gupta I, Hassanain S, Makadia J, et al. Mortality Benefit of Remdesivir in COVID-19: A Systematic Review and Meta-Analysis.
Front Med (Lausanne) 2021;7:606429. DOI: 10.3389/fmed.2020.606429 PMID: 33585508 - Jain R, Javeri Y, Nasa P, Kashyap R, Khanna Ak, Tayar Aa, et al. Consensus Statement for Pharmacological Management of Coronavirus Disease 2019 (COVID-19): A Pragmatic Approach.
Asploro J Biomed Clin Case Rep 2020;3:241. - Kirkup C, Pawlowski C, Puranik A, Conrad I, O’Horo JC, Gomaa D, et al. Healthcare disparities among anticoagulation therapies for severe COVID-19 patients in the multi-site VIRUS registry.
J Med Virol 2021;93:4303-4318. DOI: 10.1002/jmv.26918 PMID: 33666246 - Karale S, Bansal VK, Makadia J, Tayyeb M, Khan H, Ghanta S, et al. A Meta-analysis of Mortality, Need for ICU admission, Use of Mechanical Ventilation and Adverse Effects with Ivermectin Use in COVID-19 Patients.
Med Rxiv ;2021. [DOI:10.1101/2021.04.30.21256415]. - Garcia MA, Johnson SW, Bosch NA, Sisson EK, Sheldrick CR, Kumar VK, et al. Variation in Use of Repurposed Medications Among Patients With Coronavirus Disease 2019. From The Society of Critical Care Medicine Discovery Viral Infection and Respiratory Illness Universal Study: Coronavirus Disease 2019 Registry Investigator Group.
Crit Care Explor 2021;3:e0566. DOI: 10.1097/CCE.0000000000000566 PMID: 34746796 - Garcia MA, Johnson SW, Sisson EK, Sheldrick CR, Kumar VK, Boman K, et al. Variation in Use of High-Flow Nasal Cannula and Noninvasive Ventilation Among Patients With COVID-19.
Respir Care 2022;67:929- 938. DOI: 10.4187/respcare.09672 PMID: 35672139 - Bansal V, Mahapure KS, Mehra I, Bhurwal A, Tekin A, Singh R, et al. Mortality Benefit of Convalescent Plasma in COVID-19: A Systematic Review and Meta-Analysis.
Front Med (Lausanne) 2021;8:624924. DOI: 10.3389/fmed.2021.624924 PMID: 33898477 - Singh R, Rathore SS, Khan H, Bhurwal A, Sheraton M, Ghosh P, et al. Mortality and Severity in COVID-19 Patients on ACEIs and ARBs-A Systematic Review, Meta-Analysis, and Meta-Regression Analysis.
Front Med (Lausanne) 2021;8:703661. DOI: 10.3389/fmed.2021.703661 PMID: 35083229 - Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement.
PLoS Med 2009;6:e1000097. DOI: 10.1371/journal.pmed.1000097 PMID: 19621072 - Wu C, Chen X, Cai Y, Xia J, Zhou X, Xu S, et al. Risk Factors Associated With Acute Respiratory Distress Syndrome and Death in Patients With Coronavirus Disease 2019 Pneumonia in Wuhan, China.
JAMA Intern Med 2020;180:934-943. DOI: 10.1001/jamainternmed.2020.0994 PMID: 32167524 - Zhu J, Ji P, Pang J, Zhong Z, Li H, He C, et al. Clinical characteristics of 3062 COVID-19 patients: A meta-analysis.
J Med Virol 2020;92:1902- 1914. DOI: 10.1002/jmv.25884 PMID: 32293716 - Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study.
Lancet 2020;395:1054-1062. DOI: 10.1016/S0140-6736(20)30566-3 PMID: 32171076 - Li L, Huang Q, Wang DC, Ingbar DH, Wang X. Acute lung injury in patients with COVID-19 infection.
Clin Transl Med 2020;10:20-27. DOI: 10.1002/ctm2.16 PMID: 32508022 - Yang X, Yu Y, Xu J, Shu H, Xia J, Liu H, et al. (2020). Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study.
Lancet Respir Med 2020;8:475-481. DOI: 10.1016/S2213-2600(20)30079-5 PMID: 32105632 - Boopathi S, Poma AB, Kolandaivel P. (2021). Novel 2019 coronavirus structure, mechanism of action, antiviral drug promises and rule out against its treatment.
J Biomol Struct Dyn 2021;39:3409-3418. DOI: 10.1080/07391102.2020.1758788 PMID: 32306836 - Parasher A. COVID-19: Current understanding of its Pathophysiology, Clinical presentation and Treatment.
Postgrad Med J 2021;97:312-320. DOI: 10.1136/postgradmedj-2020-138577 PMID: 32978337 - Xu Z, Shi L, Wang Y, Zhang J, Huang L, Zhang C, et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome.
Lancet Respir Med 2020;8:420-422. DOI: 10.1016/S2213-2600(20)30076-X PMID: 32085846 - Chow JH, Mazzeffi MA, McCurdy MT. Angiotensin Ⅱ for the Treatment of COVID-19-Related Vasodilatory Shock.
Anesth Analg 2020;131:102- 105. DOI: 10.1213/ANE.0000000000004825 PMID: 32209811 - Hariyanto T, Kurniawan A. Tocilizumab administration is associated with the reduction in biomarkers of coronavirus disease 2019 infection.
J Med Virol 2021;93:1832-1836. DOI: 10.1002/jmv.26698 PMID: 33241872 - Hariyanto TI, Kristine E, Jillian Hardi C, Kurniawan A. Efficacy of Lopinavir/Ritonavir Compared with Standard Care for Treatment of Coronavirus Disease 2019 (COVID-19): A Systematic Review.
Infect Disord Drug Targets 2020;21:e270421187364. DOI: 10.2174/1871526520666201029125725 PMID: 33121422 - Group RC, Horby P, Lim WS, Emberson JR, Mafham M, Bell JL, et al. Dexamethasone in Hospitalized Patients with Covid-19.
N Engl J Med 2021;384:693-704. DOI: 10.1056/NEJMoa2021436 PMID: 32678530 - Salton F, Confalonieri P, Meduri GU, Santus P, Harari S, Scala R, et al. Prolonged Low-Dose Methylprednisolone in Patients With Severe COVID-19 Pneumonia.
Open Forum Infect Dis 2020;7:ofaa421. DOI: 10.1093/ofid/ofaa421 PMID: 33072814 - Beigel JH, Tomashek KM, Dodd LE, Mehta AK, Zingman BS, Kalil AC, et al. Remdesivir for the Treatment of Covid-19 - Final Report.
N Engl J Med 2020;383:1813-1826. DOI: 10.1056/NEJMoa2007764 PMID: 32445440 - Shi Y, Wang Y, Shao C, Huang J, Gan J, Huang X, et al. COVID-19 infection: the perspectives on immune responses.
Cell Death Differ 2020;27:1451-1454. DOI: 10.1038/s41418-020-0530-3 PMID: 32205856 - Matthay MA, Aldrich JM, Gotts JE. Treatment for severe acute respiratory distress syndrome from COVID-19.
Lancet Respir Med 2020;8:433-434. DOI: 10.1016/S2213-2600(20)30127-2 PMID: 32203709 - Wang J, Hajizadeh N, Moore EE, McIntyre RC, Moore PK, Veress LA, et al. Tissue plasminogen activator (tPA) treatment for COVID-19 associated acute respiratory distress syndrome (ARDS): A case series.
J Thromb Haemost 2020;18:1752-1755. DOI: 10.1111/jth.14828 PMID: 32267998 - Thachil J. The versatile heparin in COVID-19.
J Thromb Haemost 2020;18:1020-1022. DOI: 10.1111/jth.14821 PMID: 32239799 - Berlin DA, Gulick RM, Martinez FJ. Severe Covid-19.
N Engl J Med 2020;383:2451-2460. DOI: 10.1056/NEJMcp2009575 PMID: 32412710 - Wang K, Zhao W, Li J, Shu W, Duan J. The experience of high-flow nasal cannula in hospitalized patients with 2019 novel coronavirusinfected pneumonia in two hospitals of Chongqing, China.
Ann Intensive Care 2020;10:37. DOI: 10.1186/s13613-020-00653-z PMID: 32232685 - Nicola M, O’Neill N, Sohrabi C, Khan M, Agha M, Agha R. Evidence based management guideline for the COVID-19 pandemic - Review article.
Int J Surg 2020;77:206-216. DOI: 10.1016/j.ijsu.2020.04.001 PMID: 32289472 - MacLaren G, Fisher D, Brodie D. Preparing for the Most Critically Ill Patients With COVID-19: The Potential Role of Extracorporeal Membrane Oxygenation.
Jama-J Am Med Assoc 2020;323:1245-1246. DOI: 10.1001/jama.2020.2342 PMID: 32074258 - Namendys-Silva SA. ECMO for ARDS due to COVID-19.
Heart Lung 2020;49:348-349. DOI: 10.1016/j.hrtlng.2020.03.012 PMID: 32223988 - . World Health O. Clinical management of severe acute respiratory infection (SARI) when COVID-19 disease is suspected: interim guidance, 13 March 2020. Geneva: World Health Organization, 2020.
- Fan E, Beitler JR, Brochard L, Calfee CS, Ferguson ND, Slutsky AS, et al. COVID-19-associated acute respiratory distress syndrome: is a different approach to management warranted?
Lancet Respir Med 2020;8:816-821. DOI: 10.1016/S2213-2600(20)30304-0 PMID: 32645311 - Shen C, Wang Z, Zhao F, Yang Y, Li J, Yuan J, et al. Treatment of 5 Critically Ill Patients With COVID-19 With Convalescent Plasma.
Jama-J Am Med Assoc 2020;323:1582-1589. DOI: 10.1001/jama.2020.4783 PMID: 32219428 - Agarwal A, Mukherjee A, Kumar G, Chatterjee P, Bhatnagar T, Malhotra P. PLACID Trial Collaborators. Convalescent plasma in the management of moderate COVID-19 in adults in India: open label phase Ⅱ multicentre randomised controlled trial (PLACID Trial).
BMJ 2020;371:m3939. DOI: 10.1136/bmj.m3939 PMID: 33093056 - Chen JY, Qiao K, Liu F, Wu B, Xu X, Jiao GQ, et al. Lung transplantation as therapeutic option in acute respiratory distress syndrome for coronavirus disease 2019-related pulmonary fibrosis.
Chin Med J (Engl) 2020;133:1390-1396. DOI: 10.1097/CM9.0000000000000839 PMID: 32251003 - Lang C, Jaksch P, Hoda MA, Lang G, Staudinger T, Tschernko E, et al. Lung transplantation for COVID-19-associated acute respiratory distress syndrome in a PCR-positive patient.
Lancet Respir Med 2020;8:1057- 1060. DOI: 10.1016/S2213-2600(20)30361-1 PMID: 32857987 - Aghagoli G, Gallo Marin B, Soliman LB, Sellke FW. Cardiac involvement in COVID-19 patients: Risk factors, predictors, and complications: A review.
J Card Surg 2020;35:1302-1305. DOI: 10.1111/jocs.14538 PMID: 32306491 - Chang WT, Toh HS, Liao CT, Yu WL. Cardiac Involvement of COVID-19: A Comprehensive Review.
Am J Med Sci 2021;361:14-22. DOI: 10.1016/j.amjms.2020.10.002 PMID: 33187633 - Tersalvi G, Vicenzi M, Calabretta D, Biasco L, Pedrazzini G, Winterton D. Elevated Troponin in Patients with Coronavirus Disease 2019: Possible Mechanisms.
J Card Fail 2020;26:470-475. DOI: 10.1016/j.cardfail.2020.04.009 PMID: 32315733 - Manolis AS, Manolis AA, Manolis TA, Apostolopoulos EJ, Papatheou D, Melita H. COVID-19 infection and cardiac arrhythmias.
Trends Cardiovasc Med 2020;30:451-460. DOI: 10.1016/j.tcm.2020.08.002 PMID: 32814095 - Chen T, Wu D, Chen H, et al. Clinical characteristics of 113 deceased patients with coronavirus disease 2019: retrospective study.
BMJ 2020;368:m1091. DOI: 10.1136/bmj.m1091 PMID: 32217556 - Talasaz AH, Kakavand H, Van Tassell B, Aghakouchakzadeh M, Sadeghipour P, Dunn S, et al. Cardiovascular Complications of COVID-19: Pharmacotherapy Perspective.
Cardiovasc Drugs Ther 2021;35:249-259. DOI: 10.1007/s10557-020-07037-2 PMID: 32671601 - Madjid M, Safavi Naeini P, Solomon SD, Vardeny O. Potential Effects of Coronaviruses on the Cardiovascular System: A Review.
JAMA Cardiol 2020;5:831-840. DOI: 10.1001/jamacardio.2020.1286 PMID: 32219363 - Geng YJ, Wei ZY, Qian HY, Huang J, Lodato R, Castriotta RJ. Pathophysiological characteristics and therapeutic approaches for pulmonary injury and cardiovascular complications of coronavirus disease 2019.
Cardiovasc Pathol 2020;47:107228. DOI: 10.1016/j.carpath.2020.107228 PMID: 32375085 - Cheng H, Wang Y, Wang GQ. Organ-protective effect of angiotensinconverting enzyme 2 and its effect on the prognosis of COVID-19.
J Med Virol 2020;92:726-730. DOI: 10.1002/jmv.25785 PMID: 32221983 - Wang JZ, Zhang RY, Bai J. An anti-oxidative therapy for ameliorating cardiac injuries of critically ill COVID-19-infected patients.
Int J Cardiol 2020;312:137-138. DOI: 10.1016/j.ijcard.2020.04.009 PMID: 32321655 - Sawalha K, Abozenah M, Kadado AJ, Battisha A, Al-Akchar M, Salerno C, et al. Systematic Review of COVID-19 Related Myocarditis: Insights on Management and Outcome.
Cardiovasc Revasc Med 2021;23:107- 113. DOI: 10.1016/j.carrev.2020.08.028 PMID: 32847728 - Force for the management of COVID-19 of the European Society of Cardiology. ESC guidance for the diagnosis and management of cardiovascular disease during the COVID-19 pandemic: part 2-care pathways, treatment, and follow-up.
Eur Heart J 2022;43:1059-1103. DOI: 10.1093/eurheartj/ehab697 PMID: 34791154 - Giudicessi JR, Noseworthy PA, Friedman PA, Ackerman MJ. Urgent Guidance for Navigating and Circumventing the QTc-Prolonging and Torsadogenic Potential of Possible Pharmacotherapies for Coronavirus Disease 19 (COVID-19).
Mayo Clin Proc 2020;95:1213-1221. DOI: 10.1016/j.mayocp.2020.03.024 PMID: 32359771 - Zhang XL, Li ZM, Ye JT, Lu J, Ye LL, Zhang CX, et al. Pharmacological and cardiovascular perspectives on the treatment of COVID-19 with chloroquine derivatives.
Acta Pharmacol Sin 2020;41:1377-1386. DOI: 10.1038/s41401-020-00519-x PMID: 32968208 - Denson JL, Gillet AS, Zu Y, Brown M, Pham T, Yoshida Y, et al. Metabolic Syndrome and Acute Respiratory Distress Syndrome in Hospitalized Patients With COVID-19.
JAMA Netw Open 2021;4:e2140568. DOI: 10.1001/jamanetworkopen.2021.40568 PMID: 34935924 - Mehta P, McAuley DF, Brown M, Sanchez E, Tattersall RS, Manson JJ. HLH Across Speciality Collaboration, UK. COVID-19: consider cytokine stor m syndromes and immunosuppression.
Lancet 2020;395:1033-1034. DOI: 10.1016/S0140-6736(20)30628-0 PMID: 32192578 - Hu B, Huang S, Yin L. The cytokine storm and COVID-19.
J Med Virol 2021;93:250-256. DOI: 10.1002/jmv.26232 PMID: 32592501 - Anka AU, Tahir MI, Abubakar SD, Alsabbagh M, Zian Z, Hamedifar H, et al. Coronavirus disease 2019 (COVID-19): An overview of the immunopathology, serological diagnosis and management.
Scand J Immunol 2021;93:e12998. DOI: 10.1111/sji.12998 PMID: 33190302 - Zhang W, Zhao Y, Zhang F, Wang Q, Li T, Liu Z, et al. The use of antiinflammatory drugs in the treatment of people with severe coronavirus disease 2019 (COVID-19): The Perspectives of clinical immunologists from China.
Clin Immunol 2020;214:108393. DOI: 10.1016/j.clim.2020.108393 PMID: 32222466 - Klopfenstein T, Zayet S, Lohse A, Balblanc JC, Badie J, Royer PY, et al. HNF Hospital Tocilizumab multidisciplinary team. Tocilizumab therapy reduced intensive care unit admissions and/or mortality in COVID-19 patients.
Med Mal Infect 2020;50:397-400. DOI: 10.1016/j.medmal.2020.05.001 PMID: 32387320 - Amer M, Kamel AM, Bawazeer M, Maghrabi K, Butt A, Dahhan T, et al. Society of Critical Care Medicine Discovery Viral Infection and Respiratory Illness Universal Study (VIRUS): COVID-19 Registry Investigator Group. Clinical characteristics and outcomes of critically ill mechanically ventilated COVID-19 patients receiving interleukin-6 receptor antagonists and corticosteroid therapy: a preliminary report from a multinational registry.
Eur J Med Res 2021;26:117. DOI: 10.1186/s40001-021-00591-x PMID: 34600589 - Salama C, Han J, Yau L, Reiss WG, Kramer B, Neidhart JD, et al. Tocilizumab in Patients Hospitalized with COVID-19 Pneumonia.
N Engl J Med 2021;384:20-30. DOI: 10.1056/NEJMoa2030340 PMID: 33332779 - Luo P, Liu Y, Qiu L, Liu X, Liu D, Li J. Tocilizumab treatment in COVID-19: A single center experience.
J Med Virol 2020;92:814-818. DOI: 10.1002/jmv.25801 PMID: 32253759 - Ma J, Xia P, Zhou Y, Liu Z, Zhou X, Wang J, et al. Potential effect of blood purification therapy in reducing cytokine storm as a late complication of critically ill COVID-19.
Clin Immunol 2020;214:108408. DOI: 10.1016/j.clim.2020.108408 PMID: 32247038 - Xie H, Zhao J, Lian N, Lin S, Xie Q, Zhuo H. Clinical characteristics of non-ICU hospitalized patients with coronavirus disease 2019 and liver injury: A retrospective study.
Liver Int 2020;40:1321-1326. DOI: 10.1111/liv.14449 PMID: 32239591 - Zhang B, Zhou X, Qiu Y, Song Y, Feng F, Feng J, et al. Clinical characteristics of 82 cases of death from COVID-19.
PLoS One 2020;15:e0235458. DOI: 10.1371/journal.pone.0235458 PMID: 32645044 - Patel KP, Patel PA, Vunnam RR, Hewlett AT, Jain R, Jing R, et al. Gastrointestinal, hepatobiliary, and pancreatic manifestations of COVID-19.
J Clin Virol 2020;128:104386. DOI: 10.1016/j.jcv.2020.104386 PMID: 32388469 - Xu L, Liu J, Lu M, Yang D, Zheng X. Liver injury during highly pathogenic human coronavirus infections.
Liver Int 2020;40:998-1004. DOI: 10.1111/liv.14435 PMID: 32170806 - Wang F, Wang H, Fan J, Zhang Y, Wang H, Zhao Q. Pancreatic Injury Patterns in Patients with Coronavirus Disease 19 Pneumonia.
Gastroenterology 2020;159:367-370. DOI: 10.1053/j.gastro.2020.03.055 PMID: 32247022 - Chai X, Hu L, Zhang Y, Han W, Lu Z, Ke AW, et al. Specific ACE2 Expression in Cholangiocytes May Cause Liver Damage After 2019-nCoV Infection.
bioRxiv :2020. DOI:https://doi.org/10.1101/2020.02.03.931766 - Boettler T, Newsome PN, Mondelli MU, Maticic M, Cordero E, Cornberg M, et al. Care of patients with liver disease during the COVID-19 pandemic: EASL-ESCMID position paper.
JHEP Rep 2020;2:100113. DOI: 10.1016/j.jhepr.2020.100113 PMID: 32289115 - Castro RA, Frishman WH. Thrombotic Complications of COVID-19 Infection: A Review.
Cardiol Rev 2021;29:43-47. DOI: 10.1097/CRD.0000000000000347 PMID: 32947478 - Wang YD, Zhang SP, Wei QZ, Zhao MM, Mei H, Zhang ZL, et al. [COVID-19 complicated with DIC: 2 cases report and literatures review].
Zhonghua Xue Ye Xue Za Zhi 2020;41:245-247. - Carfora V, Spiniello G, Ricciolino R, Di Mauro M, Migliaccio MG, Mottola FF, et al. Anticoagulant treatment in COVID-19: a narrative review.
J Thromb Thrombolysis 2021;51:642-648. DOI: 10.1007/s11239-020-02242-0 PMID: 32809158 - Barrett CD, Moore HB, Yaffe MB, Moore EE. ISTH interim guidance on recognition and management of coagulopathy in COVID-19: A comment.
J Thromb Haemost 2020;18:2060-2063. DOI: 10.1111/jth.14860 PMID: 32302462 - Harenberg J, Favaloro E. COVID-19: progression of disease and intravascular coagulation-present status and future perspectives.
Clin Chem Lab Med 2020;58:1029-1036. DOI: 10.1515/cclm-2020-0502 PMID: 32406381 - Billett HH, Reyes-Gil M, Szymanski J, Ikemura K, Stahl LR, Lo Y, et al. Anticoagulation in COVID-19: Effect of Enoxaparin, Heparin, and Apixaban on Mortality.
Thromb Haemost 2020;120:1691-1699. DOI: 10.1055/s-0040-1720978 PMID: 33186991 - Shi C, Tingting W, Li JP, et al. Comprehensive Landscape of Heparin Therapy for COVID-19.
Carbohydr Polym 2021;254:117232. DOI: 10.1016/j.carbpol.2020.117232 PMID: 33357843 - Asadi-Pooya AA, Simani L. Central nervous system manifestations of COVID-19: A systematic review.
J Neurol Sci 2020;413:116832. DOI: 10.1016/j.jns.2020.116832 PMID: 32299017 - Mao L, Jin H, Wang M, Hu Y, Chen S, He Q, et al. Neurologic Manifestations of Hospitalized Patients with Coronavirus Disease 2019 in Wuhan, China.
JAMA Neurol 2020;77:683-690. DOI: 10.1001/jamaneurol.2020.1127 PMID: 32275288 - Sedaghat Z, Karimi N. Guillain Barre syndrome associated with COVID-19 infection: A case report.
J Clin Neurosci 2020;76:233-235. DOI: 10.1016/j.jocn.2020.04.062 PMID: 32312628 - Pleasure SJ, Green AJ, Josephson SA. The Spectrum of Neurologic Disease in the Severe Acute Respiratory Syndrome Coronavirus 2 Pandemic Infection: Neurologists Move to the Frontlines.
JAMA Neurol 2020;77:679-680. DOI: 10.1001/jamaneurol.2020.1065 PMID: 32275291 - Jin H, Hong C, Chen S, Zhou Y, Wang Y, Mao L, et al. Consensus for prevention and management of coronavirus disease 2019 (COVID-19) for neurologists.
Stroke Vasc Neurol 2020;5:146-151. DOI: 10.1136/svn-2020-000382 PMID: 32385132 - Cheng Y, Luo R, Wang K, Zhang M, Wang Z, Dong L, et al. Kidney disease is associated with in-hospital death of patients with COVID-19.
Kidney Int 2020;97:829-838. []PMID: 32247631 DOI: 10.1016/j.kint.2020.03.005. - Adapa S, Aeddula NR, Konala VM, Chenna A, Naramala S, Madhira BR, et al. COVID-19 and Renal Failure: Challenges in the Delivery of Renal Replacement Therapy.
J Clin Med Res 2020;12:276-285. DOI: 10.14740/jocmr4160 PMID: 32489502 - Yang XH, Sun RH, Chen DC. [Diagnosis and treatment of COVID-19: acute kidney injury cannot be ignored].
Zhonghua Yi Xue Za Zhi 2020;100:1205-1208. - Walkey AJ, Kumar VK, Harhay MO, Bolesta S, Bansal V, et al. The Viral Infection and Respiratory Illness Universal Study (VIRUS): An International Registry of Coronavirus 2019-Related Critical Illness.
Crit Care Explor 2020;2:e0113. DOI: 10.1097/CCE.0000000000000113 PMID: 32426754 - Walkey AJ, Sheldrick RC, Kashyap R, Kumar VK, Boman K, Bolesta S, et al. Guiding Principles for the Conduct of Observational Critical Care Research for Coronavirus Disease 2019 Pandemics and Beyond: The Society of Critical Care Medicine Discovery Viral Infection and Respiratory Illness Universal Study Registry.
Crit Care Med 2020;48:e1038-e1044. DOI: 10.1097/CCM.0000000000004572 PMID: 32932348