ABSTRACT
Objective: To analyze the levels of structural variation and forecasting of medical costs in public hospitals in China between 2010 and 2020. Methods: We analyzed the changes in average per-outpatient visit cost and average per-treatment cost of public hospitals at each level in China using the degree of structural variation, and forecasted the medical costs of public hospitals from 2021 to 2025 using a GM(1,1) model. Results: Between 2010 and 2020, the rate of contribution of medication costs was the highest at public hospitals of all levels, and the rate of contribution of other costs in public hospitals of all levels exhibited an upward fluctuation. Conclusion: Medical costs in Chinese public hospitals have been controlled effectively, but there is still much room for reducing the proportion of outpatient costs attributed to medication. In addition, controlling the cost of consumables should be prioritized to break the current pattern of medical service price shifting caused by regulating the proportion of individual costs, and to optimize the revenue structure of hospitals. Different levels of hospitals have different changes in cost structures, and promoting coordinated development of hospitals of all levels is necessary.
Key words: public hospitals, medical costs, levels of structural change, GM(1, 1) model
INTRODUCTION
Since the 2009 healthcare system reform in China, public hospitals have gradually expanded and the increase in medical costs has decelerated. However, the problem of unreasonable increases in medical costs continues to exist. Therefore, we gathered information from the China Public Health Statistical Yearbook regarding public hospitals, including the amount and percentage of their medical expenses at all levels of hospitals. Using structural variation analysis and the GM(1,1) forecasting model, we examined the extent, importance, and pace of change in the proportion of medical costs at public hospitals of all levels. We also forecasted the medical costs of public hospitals and their proportions in the next five years. We studied the structural variations and future trends of Chinese public hospitals’ medical costs to provide a reference for cost structure optimization and rational control of growing costs.
DATA SOURCES AND METHODS
Data sources
The data in the study were collected from the “China Public Health Statistical Yearbooks 2011–2021”. This resource lists the medical expenses of public and other hospitals of all levels in China between 2010 and 2020, including the average cost per outpatient visit, the average cost per inpatient visit, and the average inpatient cost per visit. Between 2010 and 2020, the number of public hospitals in China decreased from 13,850 to 11,870, among which tertiary public hospitals continued to grow, from 1,258 to 2,588, secondary hospitals decreased from 6,104 to 5,833, and primary hospitals exhibited a downward fluctuation, from 3,081 to 2,267.
Methods
Degree of structural variation. The degree of structural variation is a dynamic data processing method that is an overall expression of the changes in the composition of the internal structure of health care costs. It is measured on a scale of 0% to 100%, with higher values indicating a greater level of structural change of the corresponding component.[1] The value of structural variation (VSV) is the difference in values of each component at the end and beginning of the period. Its sign reflects the direction of change of each component during the period. The degree of structural variation (DSV) is the sum of the absolute differences between the component values at the end and beginning of the period. The rate of contribution to structural variation reflects the influence of the component proportion on DSV.[2] These are calculated as follows.
VSV = Xi0-Xi1
DSV = ∑|Xi1- Xi0|
Rate of contribution to structural variation = |Xi1- Xi0| / DSV * 100%
This study examined how individual costs impact structural variation in outpatient and inpatient costs at public hospitals in China from 2010 to 2019. The study calculated the VSV, DSV, and rate of contribution to the variation in average cost per outpatient and inpatient visit at primary, secondary, and tertiary hospitals.
GM(1,1) model
The GM(1,1) model is a type of gray forecasting model used to predict irregular sequences. Gray forecasting models predict irregular original gray sequences by constructing differential equations for the sequences. They are among the most widely used models in the hospital health field because of their small sample size requirements, convenience, and high short-term forecasting accuracy.[3]
The basic steps to construct a GM(1,1) model are to generate the sequence X by accumulating the original data sequence, define the gray derivatives and gray differential equations based on the generated sequence, use the least squares method to find the development coefficients a and gray variables b, establish the model and time response equations, calculate the forecasted values, and test the model.[4] The time response equation and the reduced value of the GM(1,1) prediction model are as follows.


RESULTS
General characteristics
To exclude the effect of CPI, the GDP deflator was used to adjust the costs of healthcare in 2011–2020, using 2010 as the baseline period. The results show that medical costs have increased since 2010, with an average annual growth rate of 6.44% for the average cost per outpatient visit and 5.62% for the average cost per inpatient visit. Between 2010 and 2020, outpatient medication costs were the highest compared to other costs (Table 1). While this proportion decreases gradually, it remains the main component of outpatient expenses. The proportion of examination costs decreased sharply in 2012 and then gradually increased. The proportion of other costs, primarily consumables, has increased year over year. The cost of medication as a proportion of inpatient costs has decreased significantly to 25.99% in 2020. The proportion of examination costs decreased significantly in 2012, as surgery costs were separated from examination costs starting in 2011. The proportion of surgery costs did not change significantly, whereas other costs increased year over year and became the principal component of inpatient costs.
| Year | Average outpatient visit cost (CNY) | Proportion (%) | Average inpatient visit cost (CNY) | Proportion (%) | |||||
| Medicines | Exams | Other | Medicines | Exams | Surgeries | Other | |||
| 2010 | 167.30 | 52.24 | 29.47 | 18.29 | 6415.90 | 43.40 | 25.94 | 8.31 | 22.35 |
| 2011 | 170.98 | 51.50 | 29.69 | 18.81 | 6556.46 | 42.02 | 26.65 | 7.91 | 23.42 |
| 2012 | 178.85 | 51.34 | 18.72 | 29.94 | 6774.17 | 41.32 | 7.72 | 6.51 | 44.45 |
| 2013 | 187.38 | 50.22 | 18.61 | 31.17 | 7083.32 | 39.65 | 8.01 | 6.21 | 46.12 |
| 2014 | 195.81 | 49.32 | 18.86 | 31.81 | 7325.76 | 38.44 | 8.26 | 6.01 | 47.28 |
| 2015 | 204.96 | 48.34 | 18.84 | 32.82 | 7697.29 | 36.90 | 8.53 | 5.89 | 48.67 |
| 2016 | 210.60 | 46.69 | 19.03 | 34.28 | 7885.33 | 34.62 | 8.72 | 6.10 | 50.55 |
| 2017 | 216.21 | 43.99 | 19.29 | 36.72 | 8042.09 | 30.91 | 9.04 | 6.69 | 53.36 |
| 2018 | 224.19 | 42.17 | 19.47 | 38.35 | 8216.85 | 27.88 | 9.46 | 7.07 | 55.59 |
| 2019 | 230.19 | 42.04 | 19.51 | 38.46 | 8391.51 | 27.23 | 9.74 | 7.37 | 55.67 |
| 2020 | 250.05 | 40.54 | 20.11 | 39.35 | 8874.58 | 25.99 | 9.96 | 7.78 | 56.27 |
Structural variation in medical costs
VSV and DSV of average per-outpatient visit cost: Between 2010 and 2020, the structural variation of annual per-visit outpatient cost in tertiary public hospitals was 2.61%. The VSV scores show the direction of change for each cost component. Medication costs have decreased (negative VSV), while other costs have increased (positive VSV) year over year. Examination costs have generally positive structural variation, among which the DSV in 2016–2017 was the greatest. The average annual DSV of outpatient costs in secondary public hospitals was 2.28%. The VSV of medication costs was positive in 2018–2019 but negative in all other years. The structural variation of examination costs alternated between positive and negative, whereas that of other costs was always positive, with the largest DSV in 2016–2017. The average annual DSV of outpatient costs in primary public hospitals was 1.63%, and the structural variation in medication, examination, and other costs generally exhibited alternating positive and negative variations, with the largest DSV of 4.10% in 2015–2016 (Table 2, Figures 1–3).
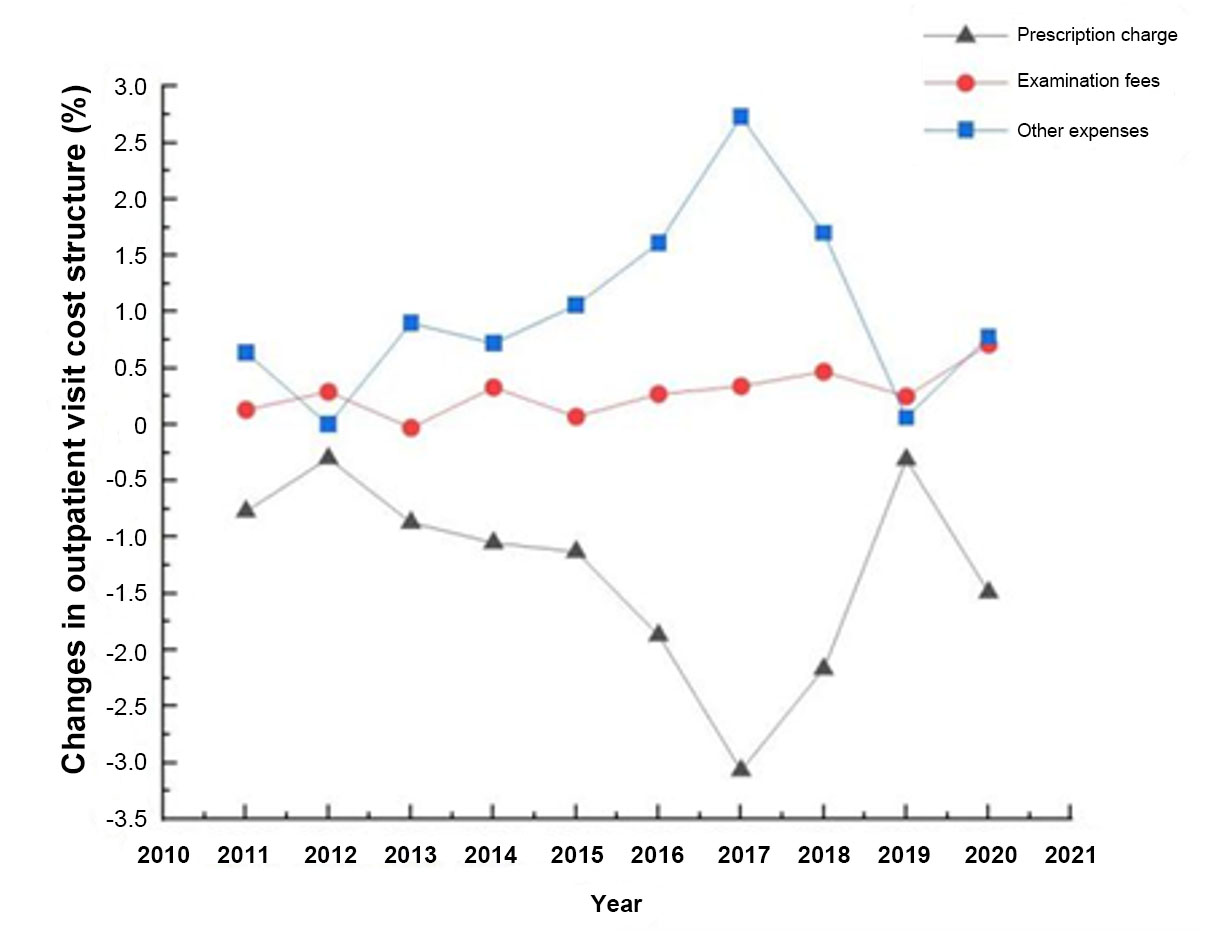
Figure 1. Changes in outpatient visit cost structure at public tertiary hospitals, 2010–2020.
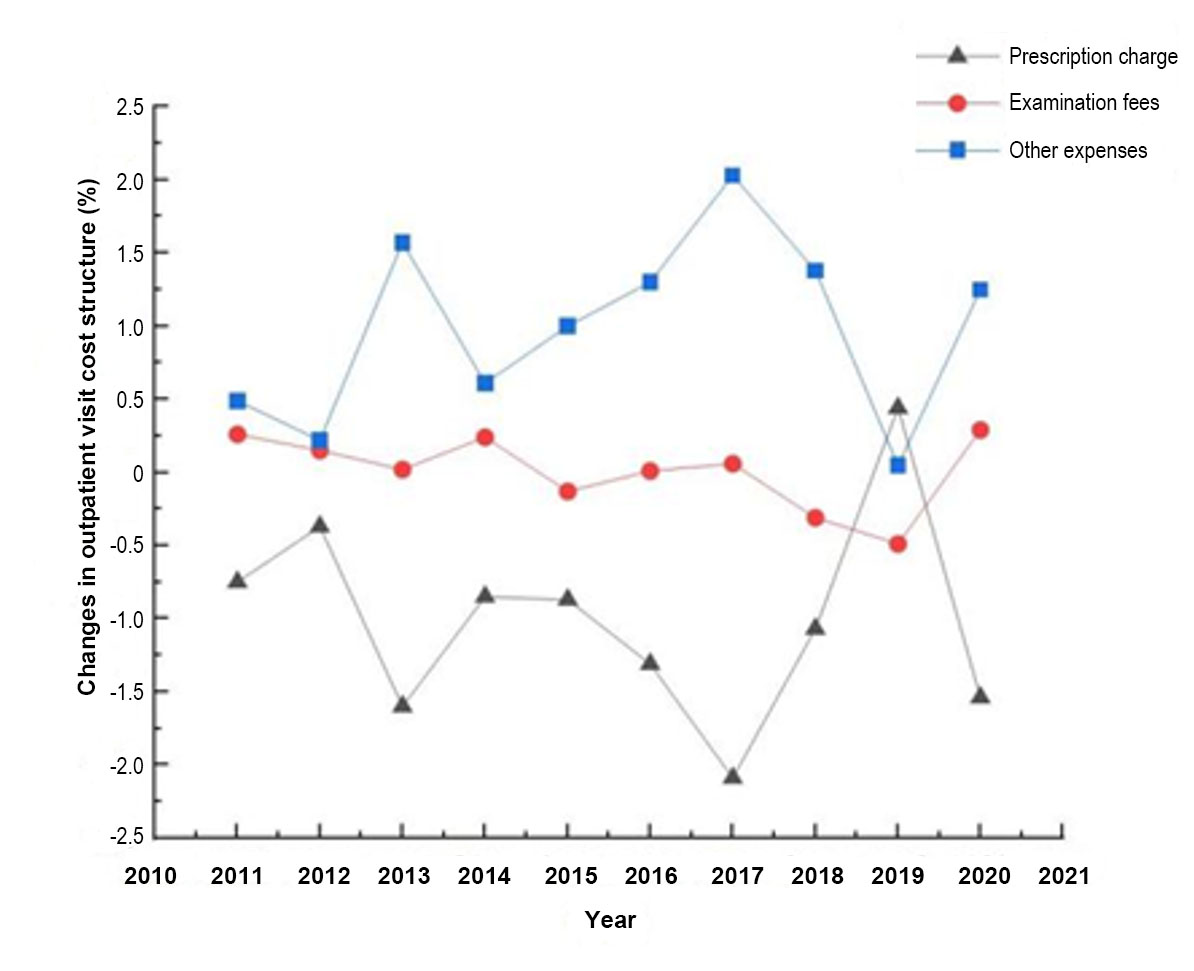
Figure 2. Changes in outpatient visit cost structure at public secondary hospitals, 2010–2020.
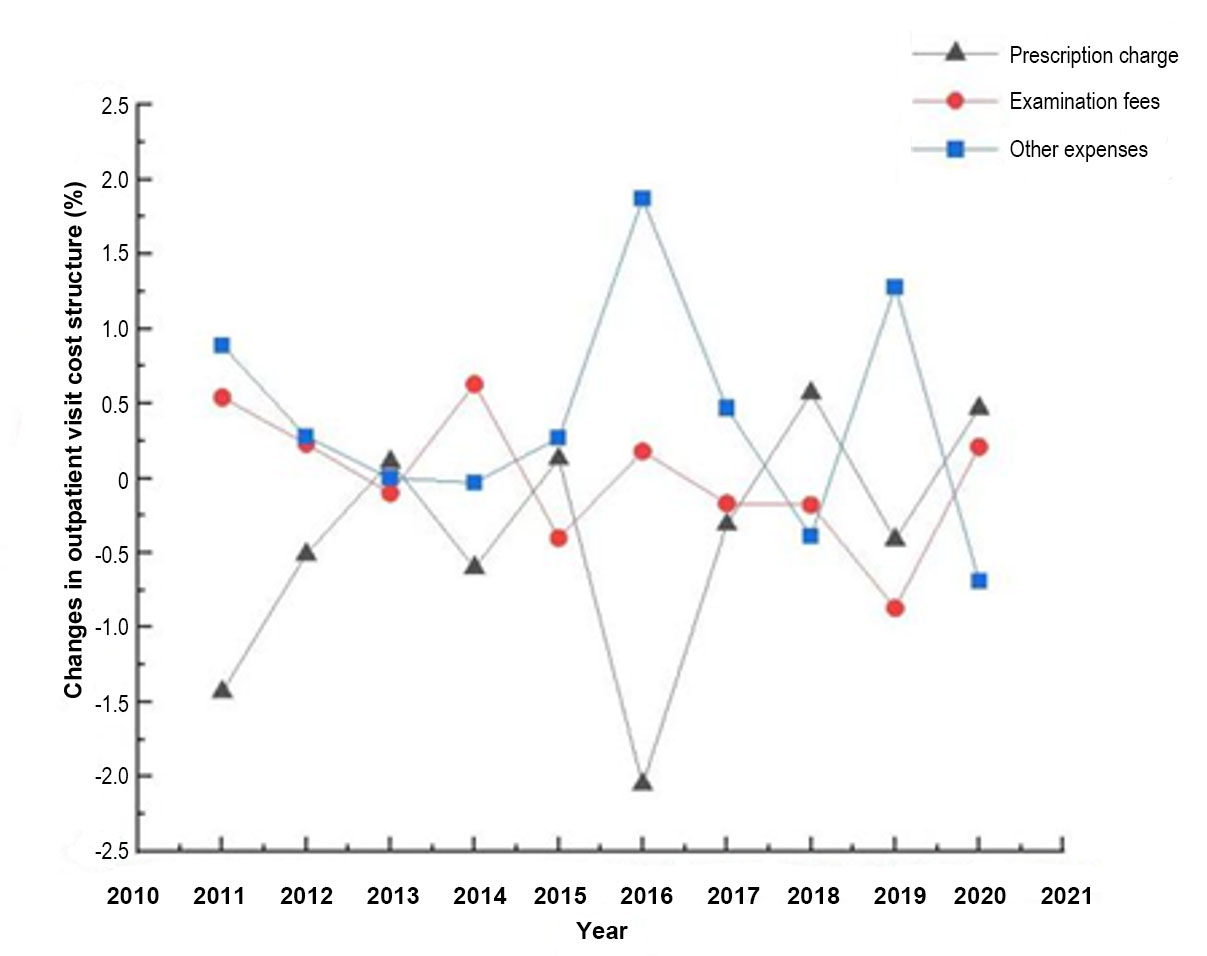
Figure 3. Changes in outpatient visit cost structure at public primary hospitals, 2010–2020.
| Year | DSV of average per-outpatient visit cost | DSV in the average cost per inpatient visit | ||||
| Tertiary hospitals | Secondary hospitals | Primary hospitals | Tertiary hospitals | Secondary hospitals | Primary hospitals | |
| 2010–2011 | 1.55 | 1.49 | 2.86 | 3.80 | 3.01 | 1.05 |
| 2011–2012 | 0.60 | 0.75 | 1.02 | 4.40 | 3.54 | 2.49 |
| 2012–2013 | 1.80 | 3.20 | 0.21 | 3.14 | 5.09 | 4.75 |
| 2013–2014 | 2.11 | 1.70 | 1.25 | 2.26 | 3.71 | 2.31 |
| 2014–2015 | 2.26 | 2.01 | 0.81 | 2.61 | 4.87 | 3.52 |
| 2015–2016 | 3.74 | 2.62 | 4.10 | 4.27 | 5.24 | 5.21 |
| 2016–2017 | 6.15 | 4.18 | 0.95 | 7.91 | 6.21 | 7.63 |
| 2017–2018 | 4.34 | 2.76 | 1.15 | 6.25 | 5.48 | 6.26 |
| 2018–2019 | 0.61 | 0.98 | 2.56 | 1.22 | 1.69 | 4.85 |
| 2019–2020 | 2.98 | 3.08 | 1.37 | 2.20 | 3.19 | 6.75 |
| 2010–2020 | 26.14 | 22.75 | 16.29 | 38.06 | 42.03 | 44.83 |
VSV and DSV in the average cost per inpatient visit: Figures 4–6 show that the VSV of medication costs among inpatient costs at secondary and tertiary public hospitals have been negative, whereas those of other costs have been positive. The VSV of examination costs at tertiary and secondary hospitals has been positive. In contrast, the VSV of examination costs at primary hospitals were negative in 2014–2015 and 2017–2018 and positive in all other years. The VSV of surgery costs at primary hospitals was always negative, whereas the VSV at secondary and tertiary hospitals alternated between positive and negative. The DSV of inpatient costs has generally increased, with the annual average DSV of inpatient costs at primary, secondary, and tertiary public hospitals being 4.48%, 4.20%, and 3.81%, respectively.
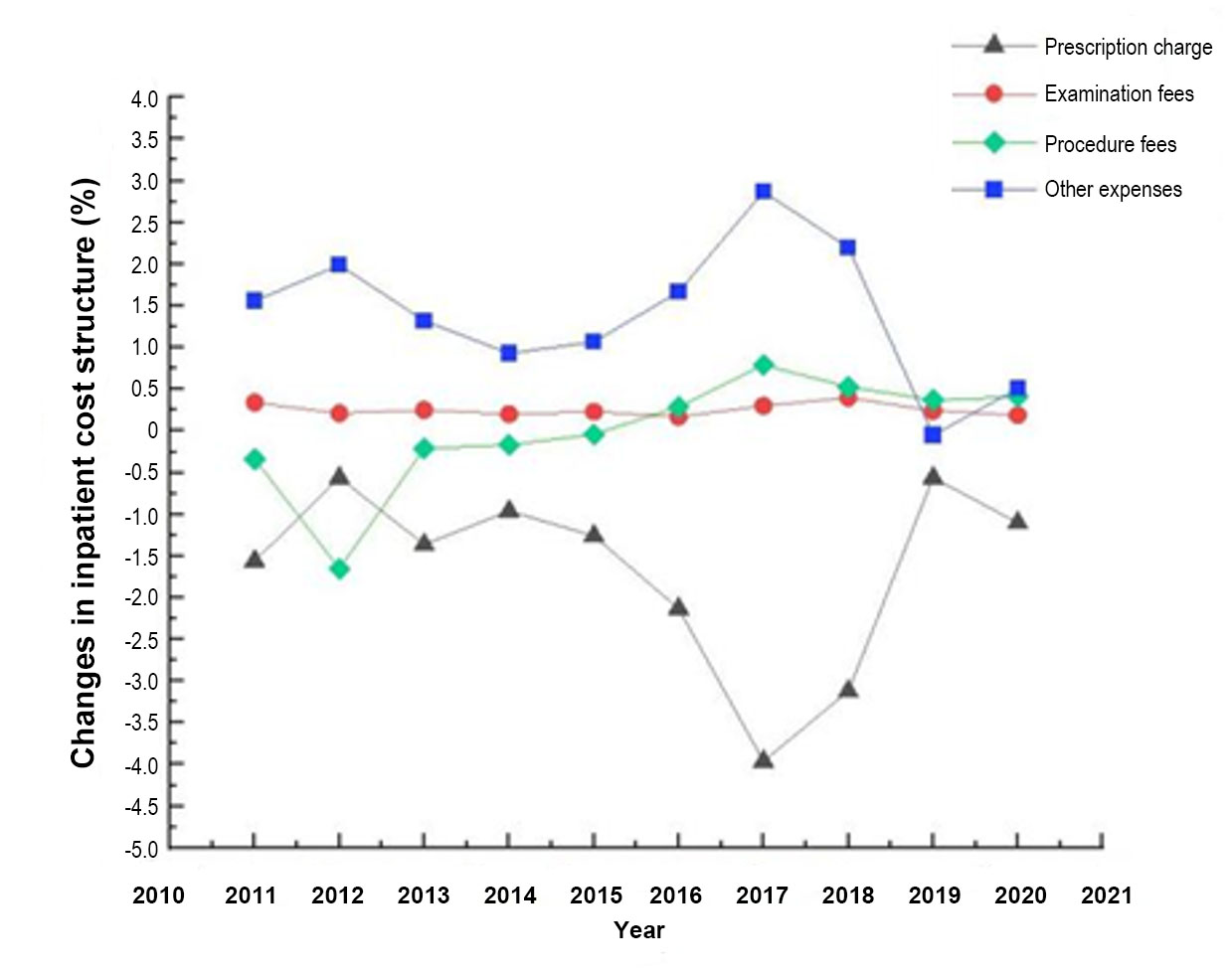
Figure 4. Changes in inpatient cost structure at public tertiary hospitals, 2010–2020.
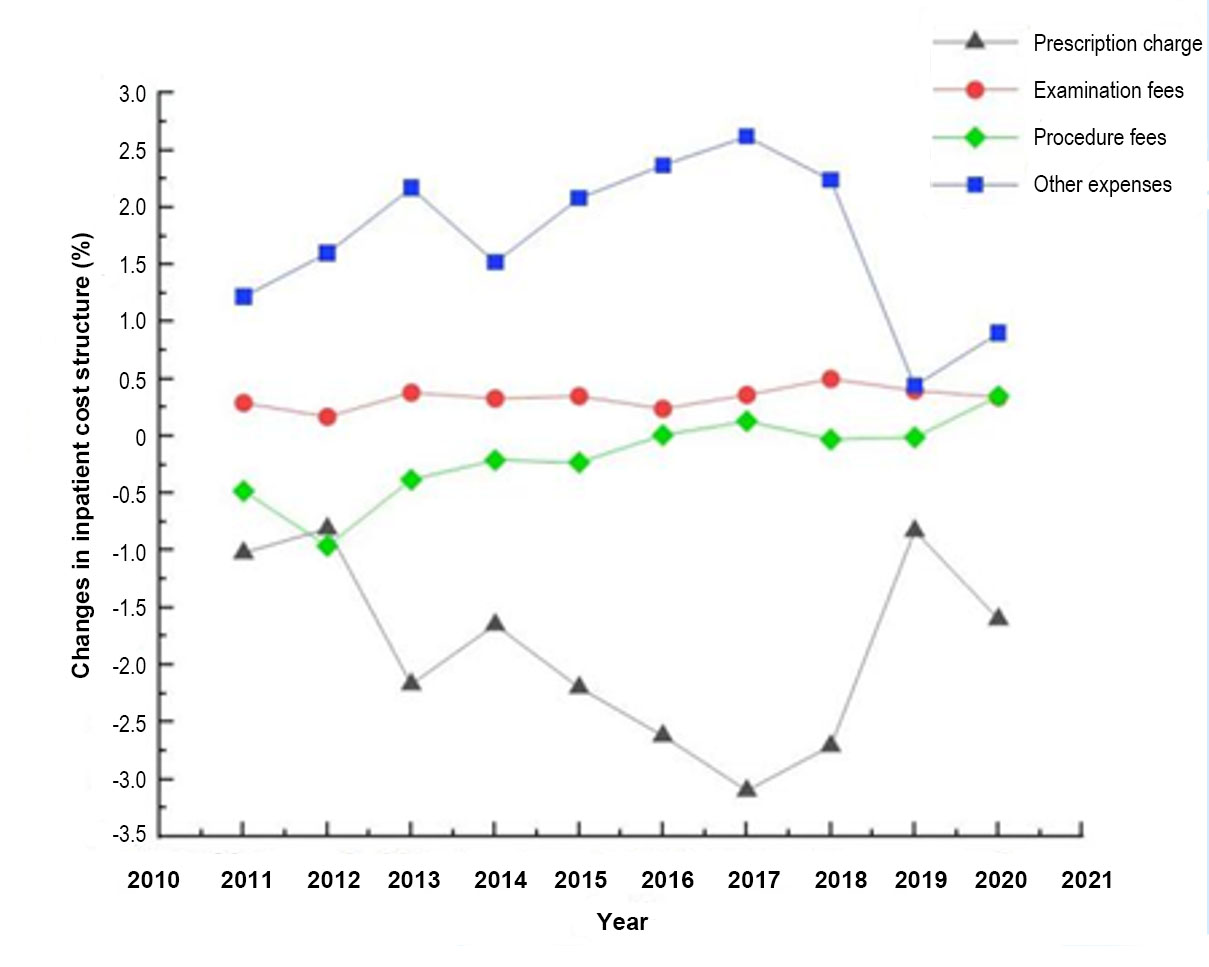
Figure 5. Changes in inpatient cost structure at public secondary hospitals, 2010–2020.
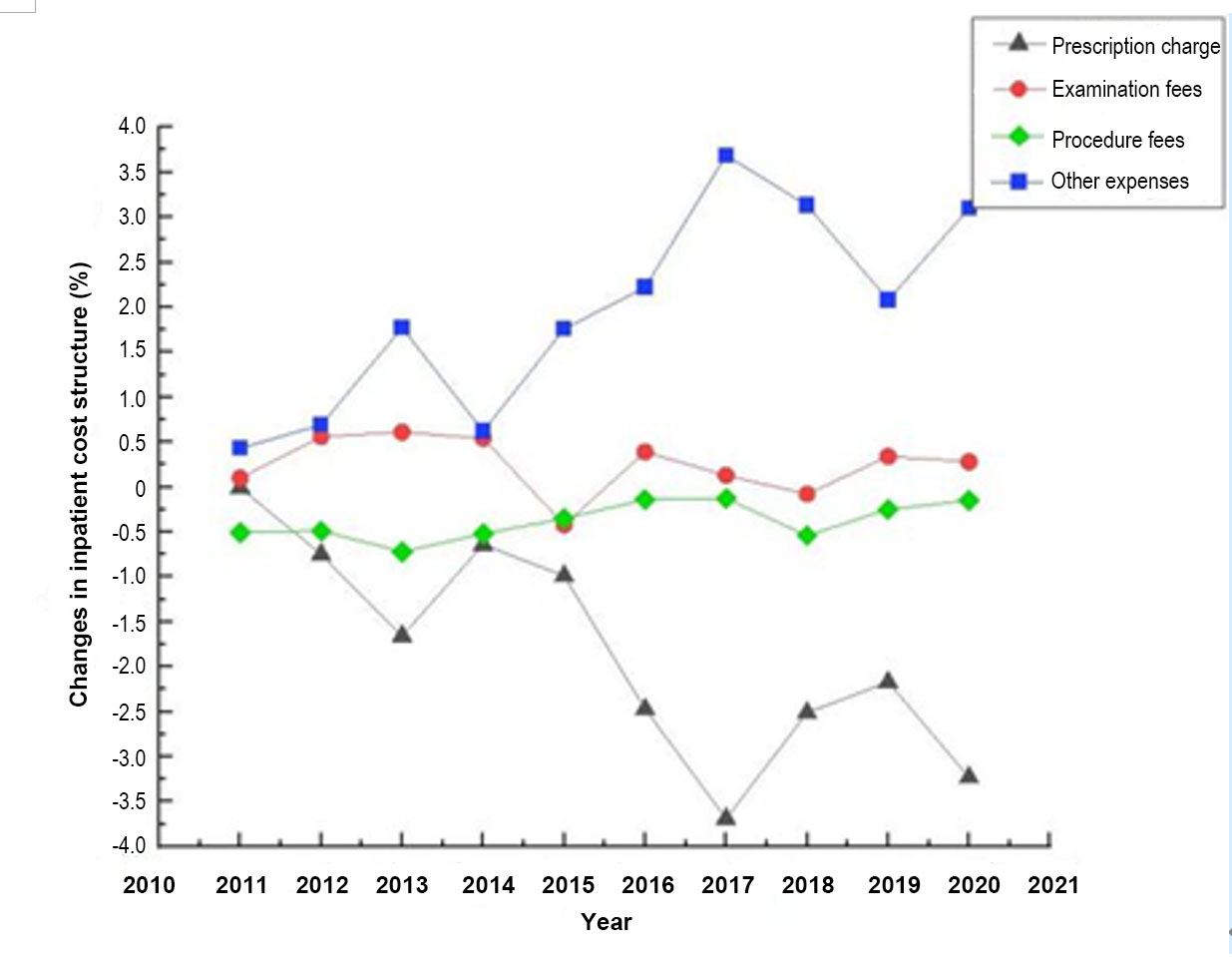
Figure 6. Changes in inpatient cost structure at public primary hospitals, 2010–2020.
Rate of contribution to outpatient cost structure variation: Table 3 shows that the primary contributor to outpatient cost variation at primary, secondary, and tertiary public hospitals in China in 2010–2020 was medication cost, at 50.00%. Furthermore, the rate of contribution of examination costs has generally increased at tertiary hospitals compared with primary and secondary hospitals. The rate of contribution of other costs to structural variation has fluctuated, and the average annual rate of contribution to structural variation has reached 30.00% or more.
| Year | Tertiary hospitals | Secondary hospitals | Primary hospitals | ||||||
| Medicines | Exams | Other | Medicines | Exams | Other | Medicines | Exams | Other | |
| 2010–2011 | 50.00 | 8.45 | 41.55 | 50.00 | 17.17 | 32.83 | 50.00 | 19.05 | 30.95 |
| 2011–2012 | 50.00 | 49.49 | 0.51 | 50.00 | 20.60 | 29.40 | 50.00 | 22.26 | 27.74 |
| 2012–2013 | 48.38 | 1.62 | 50.00 | 50.00 | 0.72 | 49.28 | 50.00 | 48.19 | 1.81 |
| 2013–2014 | 50.00 | 15.72 | 34.28 | 50.00 | 14.21 | 35.79 | 47.68 | 50.00 | 2.32 |
| 2014–2015 | 50.00 | 3.22 | 46.78 | 43.63 | 6.37 | 50.00 | 16.06 | 50.00 | 33.94 |
| 2015–2016 | 50.00 | 7.09 | 42.91 | 50.00 | 0.32 | 49.68 | 50.00 | 4.45 | 45.55 |
| 2016–2017 | 50.00 | 5.60 | 44.40 | 50.00 | 1.40 | 48.60 | 32.31 | 17.69 | 50.00 |
| 2017–2018 | 50.00 | 10.87 | 39.13 | 38.68 | 11.32 | 50.00 | 50.00 | 16.04 | 33.96 |
| 2018–2019 | 50.00 | 40.61 | 9.39 | 45.20 | 50.00 | 4.80 | 16.17 | 33.83 | 50.00 |
| 2019–2020 | 50.00 | 23.68 | 26.32 | 50.00 | 9.34 | 40.66 | 34.36 | 15.64 | 50.00 |
| 2010–2020 | 50.00 | 10.87 | 39.13 | 50.00 | 0.50 | 49.50 | 50.00 | 0.86 | 49.14 |
| Annual rate of contribution to average structural change | 49.84 | 16.63 | 33.53 | 47.75 | 13.15 | 39.10% | 39.66 | 27.71 | 32.63 |
Rate of contribution to inpatient per-visit cost structure variation: Table 4 shows that other costs are the primary contributor to inpatient per-visit cost structure variation at primary public hospitals in China in 2010–2020, at 43.44%. Medication costs are the primary contributor to inpatient per-visit cost structure variation at secondary and tertiary public hospitals, at 44.53% and 43.35%, respectively. In contrast, the rate of contribution of examination and surgery costs to inpatient per-visit cost structure variation is small, with the rate of contribution of examination and surgery costs at primary hospitals exhibiting a fluctuating decrease.
| Year | Tertiary hospitals | Secondary hospitals | Primary hospitals | |||||||||
| Medicines | Exams | Surgeries | Other | Medicines | Exams | Surgeries | Other | Medicines | Exams | Surgeries | Other | |
| 2010–2011 | 41.02 | 8.91 | 8.98 | 41.09 | 34.04 | 9.56 | 15.96 | 40.44 | 1.28 | 9.12 | 48.72 | 40.88 |
| 2011–2012 | 12.62 | 4.70 | 37.38 | 45.30 | 22.86 | 4.82 | 27.14 | 45.18 | 30.14 | 22.30 | 19.86 | 27.70 |
| 2012–2013 | 43.23 | 7.83 | 6.77 | 42.17 | 42.54 | 7.43 | 7.46 | 42.57 | 34.88 | 12.81 | 15.12 | 37.19 |
| 2013–2014 | 48.29 | 9.00 | 1.71 | 41.00 | 44.43 | 8.94 | 5.57 | 41.06 | 27.54 | 23.34 | 22.46 | 26.66 |
| 2014–2015 | 50.00 | 4.09 | 6.84 | 39.07 | 45.29 | 7.25 | 4.71 | 42.75 | 28.19 | 11.85 | 9.96 | 50.00 |
| 2015–2016 | 50.00 | 3.74 | 9.95 | 36.31 | 50.00 | 4.52 | 0.19 | 45.30 | 47.40 | 7.46 | 2.60 | 42.54 |
| 2016–2017 | 50.00 | 6.38 | 8.43 | 35.19 | 50.00 | 5.76 | 2.07 | 42.17 | 48.36 | 1.70 | 1.64 | 48.30 |
| 2017–2018 | 46.01 | 19.95 | 30.05 | 3.99 | 49.42 | 9.15 | 0.58 | 40.85 | 40.09 | 1.36 | 8.55 | 50.00 |
| 2018–2019 | 50.00 | 8.50 | 18.50 | 23.00 | 49.30 | 23.91 | 0.70 | 26.09 | 44.78 | 7.06 | 5.22 | 42.94 |
| 2019–2020 | 49.88 | 7.61 | 0.12 | 42.39 | 50.00 | 10.71 | 11.04 | 28.25 | 47.75 | 4.16 | 2.25 | 45.84 |
| 2010–2020 | 43.35 | 8.19 | 13.63 | 34.83 | 44.53 | 8.00 | 6.64 | 40.83 | 40.41 | 7.68 | 8.47 | 43.44 |
| Annual rate of contribution to average structural change | 48.29 | 9.00 | 1.71 | 41.00 | 43.79 | 9.21 | 7.54 | 39.46 | 35.04 | 10.12 | 13.64 | 41.20 |
Medical cost forecasting model
The model was tested using posterior difference tests. First, the standard deviation and residuals of the original sequences were calculated. We used this data to determine the posterior difference ratio C and the small error probability P. In addition, the accuracy of the gray forecasting model was classified based on the accuracy of the GM(1,1) model (Table 5).[5] Table 6 shows that the forecasting model has ratio C < 0.35 and P > 0.95 for the proportion of medical costs and costs other than surgical costs, with excellent model accuracy. The forecasting accuracy of the model for the proportion of surgical costs was also satisfactory, indicating the accuracy of the model.
| Degree | Level of accuracy | P value | Ratio C |
| 1 | Good | 0.95 to 1.00 | 0.00 |
| 2 | Satisfactory | 0.80 | 0.35 |
| 3 | Barely satisfactory | 0.70 | 0.50 |
| 4 | Unsatisfactory | 0.00 | > 0.65 |
| Item | Forecasting model | Test statistic C | P value | Degree of accuracy |
| Average outpatient visit cost | 2749.7239e0.063k-2597.2239 | 0.0832 | > 0.95 | Level 1 |
| Medicines | -2050.0117e-0.0265k+2102.4717 | 0.2203 | > 0.95 | Level 1 |
| Exams | 1865.1846e0.0099k-1846.4646 | 0.2655 | > 0.95 | Level 1 |
| Other | 829.1525e0.0367k-799.2125 | 0.1837 | > 0.95 | Level 1 |
| Average inpatient visit cost | 120978.2432e0.0532k-115122.0432 | 0.0860 | > 0.95 | Level 1 |
| Medicines | -888.2990e0.0523k+932.23901 | 0.2189 | > 0.95 | Level 1 |
| Exams | 244.8882e0.0321k-237.1682 | 0.0670 | > 0.95 | Level 1 |
| Surgeries | 139.1387e0.0404k-132.6287 | 0.3841 | > 0.8 | Level 2 |
| Other | 1458.2064e0.0312k-1413.7564 | 0.1834 | > 0.95 | Level 1 |
2021–2025 medical cost forecasting results
Table 6 shows that the development coefficient of each cost in the forecasting model is < 0.30, and the accuracy of 2-step and 5-step GM(1,1) forecasting was over 97.00%, making it appropriate for medium- and long-term forecasting. Therefore, the constructed model is suitable for medium- and long-term forecasting of per-visit public hospital costs in China and its composition. The forecasting results show that the medical cost per visit will increase in 2021–2025, with the average cost per outpatient visit increasing by 102.21 CNY and the average cost per inpatient visit increasing by 3,328.06 CNY in 2025 compared to 2020.
Among the components of outpatient and medical costs, the proportion of medication costs will continue to decrease, whereas the proportion of examination and surgery costs will gradually increase. The proportion of other costs in both is forecasted to increase annually, in which the proportion of other costs among outpatient costs will overtake the proportion of medication costs as the primary contributor by 2021. The forecasted results are shown in Table 7.
| Year | Average outpatient visit cost (CNY) |
Medicines
(%) |
Exams
(%) |
Other
(%) |
Average inpatient visit cost (CNY) |
Medicines
(%) |
Exams
(%) |
Surgeries (%) |
Other
(%) |
| 2021 | 331.85 | 40.06 | 20.08 | 41.57 | 11874.08 | 25.45 | 10.33 | 7.93 | 59.33 |
| 2022 | 352.49 | 39.01 | 20.28 | 43.12 | 12523.42 | 24.15 | 10.67 | 8.25 | 61.22 |
| 2023 | 374.40 | 38.00 | 20.48 | 44.74 | 13208.26 | 22.92 | 11.03 | 8.60 | 63.16 |
| 2024 | 397.68 | 37.00 | 20.69 | 46.41 | 13930.56 | 21.75 | 11.38 | 8.95 | 65.16 |
| 2025 | 422.41 | 36.03 | 20.89 | 48.14 | 14692.36 | 20.64 | 11.75 | 9.32 | 67.23 |
DISCUSSION
Effective cost controls at Chinese public hospitals
The growth rate of medical expenses in public hospitals and hospitals at all levels in China decreased from 2010–2020. The average annual growth of outpatient and inpatient costs at primary, secondary, and tertiary hospitals increased by 6.37%, 4.75%, and 4.21% and 5.22%, 3.34%, and 2.86%, respectively, in 2010–2015, and decreased by 3.94%, 2.75%, and 3.29% and 6.14%, 2.70%, and 0.93%, respectively, in 2016–2020. This shows that after the 2015 issuance of the “Opinions on Controlling Unreasonable Increases in Medical Expenses in Public Hospitals”, provincial cost-control policies have achieved some success and reduced the financial burden of medical treatment to residents. However, medical costs have rebounded slightly since then, and the reduced effectiveness of these cost-control policies warrants attention.
Among the various components of medical costs, the control of medication costs as a proportion of inpatient costs has demonstrated higher effectiveness. By 2018, the medication costs of inpatient care in public hospitals at all levels were successfully reduced to approximately 30.00%, aligning with the goal of decreasing the medication cost proportion (excluding traditional Chinese medicine tablets) in urban public hospitals, as outlined in the “Guiding Opinions on Comprehensive Reform of Urban Public Hospitals”. During this period, the government implemented policies like providing medication at no extra cost and buying medications in bulk. These policies aimed to reduce the connection between medical care and profits from selling medication. However, the analysis of structural variation indicates that medication costs at primary, secondary, and tertiary public hospitals remain the primary factor contributing to both outpatient and inpatient costs. Although the VSV of medication costs has been negative, it still has a high proportion, especially in primary public hospitals, where medication costs have long accounted for over 50.00% of outpatient costs. In 2011, the average proportion of medication costs in OECD countries was only 16.00%,[6] so there remains much opportunity for reducing medication costs among healthcare costs in China, especially at the outpatient level.
Therefore, while governmental agencies continue promoting the normalization and institutionalization of bulk medication procurement, expanding bulk procurement coverage, and reducing medication costs, they should also play the role of clinical pharmacists to audit prescriptions written by physicians to prevent acquiescing to patient demands and indiscriminately prescribing medications[6]. In addition, to control medical costs, it is necessary not only to introduce a series of policies to regulate the billing behavior of public hospitals but also to pay attention to the effectiveness of policy implementation. The effect of the current medical cost control policy is significant in the short-term but insufficient in the long-term. Therefore, governmental agencies should coordinate with health and other relevant departments to establish a medical service price management group to regularly monitor medical costs and establish a reward and punishment system to rank cost-control targets, “downgrade” hospitals at the bottom of the rankings that fail to make corrections and provide additional financial subsidies to public hospitals at the top of the rankings.
Revenue structure of public hospitals should be optimized
While medication costs have decreased as a proportion of overall medical costs, the proportions of examination and surgery costs remained unchanged. However, the proportion of other costs, mainly consumables, has significantly increased. In 2011, the percentage of non-medication expenses in inpatient costs at tertiary hospitals was greater than the percentage of medication costs. Similarly, in 2013, the proportion of non-medication expenses in inpatient costs at primary and secondary hospitals was also greater than the percentage of medication costs. According to GM(1,1) forecasting, the proportion of other costs in outpatient costs at public hospitals will exceed that of medication costs in 2021. An analysis of the effect of medical cost control in China’s public hospitals in 2013–2019 by Wang et al.[7] also showed that the revenue structure of China’s public hospitals gradually tilted toward revenue from healthcare materials. This change in revenue structure is inconsistent with the original purpose of medical cost control and public hospital reform in China, and the value of the labor of medical personnel was not considered. However, the increase in asset-to-liability ratio has prompted public hospitals to engage in profit-seeking behavior. This has led to a situation where doctors and patients have different levels of knowledge, resulting in prominent physicians recommending expensive healthcare materials to make up for lost revenue from the elimination of medication markup. Therefore, this indicates that the phenomenon of excessive medical care has not disappeared but has replaced “medical care enriching medicine” with “healthcare materials enriching medicine.” The “one-size-fits-all” cost-control model, which pursues a reduction of the proportion of individual costs, has not addressed the core problems in medical cost control, and medical costs remain high.[8]
In this context, public hospitals should not limit their cost control measures to individual costs. Instead, the government should promote centralized procurement of consumables to the most difficult phase to disrupt the phenomenon of expensive medical consumables with severely inflated prices. More importantly, it should break the current model of medical service price shifting caused by controlling the proportion of individual costs,[9] and gradually establish a fee control model with medical insurance at the center and use the quality of medical services as the criterion for reimbursement. In addition, DRG, DIP, and other reimbursement methods should be integrated for finer control. Furthermore, the revenue structure of public hospitals should be adjusted, direct intervention by administrative means should be minimized, and an economic compensation mechanism based on fees for technical labor and medical services should be established.[10] The compensation system of medical personnel should be scientifically optimized and medical treatment behavior should be regulated, which improves motivation and quality of medical service and promotes the return of medical services to a value-based approach.
Poor control of outpatient costs compared to inpatient costs
Our calculations show that the increase of outpatient costs in public hospitals and all levels of hospitals is higher than that of inpatient costs, and the proportion of medication costs will remain high, at 36.03% by 2025, indicating that outpatient costs are poorly controlled. A possible reason is that demand for outpatient services increases with the increased number of patients with chronic diseases. In an analysis of the factors influencing frequent visits of outpatients in a community hospital, Lu et al.[11] showed that patients with five or more chronic diseases were more likely to have frequent visits. In addition, patients with chronic diseases require repeated medication purchases, and factors such as insufficient development of medication availability and insufficient variety of medications in the community drive patients toward hospital outpatient clinics. Furthermore, some inpatient costs (e.g., preoperative tests) may be shifted to outpatient clinics after the health insurance payment reform,[2] which not only increases the burden on outpatient clinics but also makes outpatient cost control ineffective. Therefore, the variety of medication for common chronic diseases in the community should be increased as appropriate, the mechanism of prescription flow should be improved, and electronic prescription centers that interface with the prescription systems of medical institutions and online prescription drug sales platforms should be established[12] to provide more channels for chronic disease patients to purchase medication, to reduce the proportion of medication costs in outpatient costs. In light of the health insurance reimbursement reform, regional health insurance departments must enhance their policies to improve quality and efficiency. They should take into consideration the region's actual situation and encourage public hospitals to control costs while providing high-quality medical services to patients. This will ensure that medical institutions, health insurance agencies, and insured individuals all receive benefits.
Coordinated development of different levels of hospitals should be promoted
Chinese public hospitals have shown some effectiveness in controlling medical costs, as higher-level hospitals have a low average annual growth of medical costs. However, the growth of medical costs at primary hospitals requires attention. From the DSV results, the inpatient cost structure at tertiary hospitals is better than that at primary and secondary hospitals, and the outpatient cost structure at primary hospitals is better than that at secondary and tertiary hospitals. Analysis of the rate of contribution to structural variation showed that the VSV and rate of contribution of surgical costs are smaller at all levels of hospitals, especially at secondary hospitals. This may be because when patients require surgical treatment, they prefer primary hospitals closer to their homes if the surgery is less complex. In addition, while the government enhances the construction of primary hospitals, the quality of medical resources has declined, and patients prefer tertiary hospitals if the surgery is riskier; this is consistent with a study by Chen et al.[13] In the long run, the surgical level of secondary hospitals will decline, which not only leads to the shifting of medical expenses toward medication and examination costs in secondary hospitals but also is not conducive to the implementation of the policy of graded diagnosis and treatment. In this regard, the government should promote the coordinated development of hospitals at all levels and guide the division of labor among these hospitals according to disease severity or different stages of disease treatment. In addition, the government should help primary and secondary hospitals improve the level of medical services for common and recurrent diseases through medical cooperation and support mechanisms and the development of medical associations, to guide patients to seek rational medical treatment and promote rational changes in the medical cost structure at all levels of hospitals.
DECLARATIONS
Author contributions
All authors have accepted responsibility for the entire content of this manuscript and approved its submission.
Secondary publication declaration
This article was translated with permission from the Chinese language version first published by Modern Hospital Management.
Conflicts of interest
There is no conflict of interest among the authors.
Data sharing statement
No additional data is available.
REFERENCES
- Xu J, Mu YQ. Analysis of changes in medical cost structure of a county-level public hospital in Chongqing from 2012-2016. Zhongguo Quanke Yixue. 2017;20(S3):438–441.
- Jia BY, Han H, Huang YX. Comparative analysis of medical cost structure changes in public hospitals in Jiangsu and Zhejiang. Weisheng Jingji Yanjiu. 2022;39(5):33–36.
- Sun J, Wang QJ. Demand forecasting analysis of health resources in Guangxi based on the GM(1,1) grey system model. Weisheng Ruankexue. , 2017;31(7):25-28.
- Xin Y, Ma WS, Li H, et al. The proportion of total health expenditure to GDP in China during the 13th Five-Year Plan. Xiandai Yufang Yixue. 2018;45(10):1804–1808.
- Dai TM, Zhen TM, Song KM. Analysis and prediction of medical costs in public hospitals in Shandong Province based on the GM(1,1) gray prediction model. Weisheng Ruankexue. 2021;35(2):51–54.
- Luo M, Huang YX. Analysis of the variation of inpatient cost structure of a comprehensive tertiary hospital in Jiangsu Province from 2015 to 2019. Zhongguo Weisheng Shiye Guanli. 2022;39(4):262–264, 286.
- Wang XF, Qin XQ, Zhang YF. Analysis of the effect of medical cost control in public hospitals in China from 2013 to 2019. Weisheng Ruankexue. 2022;36(4):53–58.
- Zhang YJ, Mao ZB. The profit-seeking mechanism and optimization strategy of public hospitals in the context of zero-plus cost of drugs. Henan Shifan Daxue Xuebao. 2021;48 (1):102–112.
- Qin CX, Tian LR, Jin SX, et al. Analysis of the trends in the volume and cost of hospital visits of different levels. Nanjing Yike Daxue Xuebao. 2021;21(5):474–478.
- Luo M, Tang QR, Yan LL, et al. Analysis of inpatient costs of patients with cerebral infarction paid by disease based on the degree of structural change. Weisheng Ruankexue. 2021;35(7):48–52.
- Lu JH, Zhang N, Du Z. Analysis of factors influencing frequent visits of outpatients in a community hospital in Beijing city. Zhongguo Dangdai Yiyao. 2022;29(9):118–121.
- Liu L. Risk identification, diagnosis, and response of online prescription drug sales. Weisheng Jingji Yanjiu. 2022;39(4):19–23.
- Chen CG. Analysis of trends in medical revenue structure changes in China's secondary public hospitals from 2012-2019. Zhonguo Yiliao Guanli Keuxue. 2022;12(2):11–16.